

Summary
Brachial blood pressure (BP) measured using oscillometric devices correlates with disease endpoints such as myocardial infarction and stroke. Arterial stiffness may represent an easy surrogate marker for atherosclerotic burden using validated measurements such as pulse wave velocity and pulse wave analysis. This article discusses the relationship between office BP and ambulatory BP monitoring and the correlation of both BP measures with surrogate markers of disease.
- Hypertensive Disease
Brachial blood pressure (BP) measured using oscillometric devices correlates with disease endpoints such as myocardial infarction (MI) and stroke. Arterial stiffness may represent an easy surrogate marker for atherosclerotic burden using validated measurements such as pulse wave velocity (PWV) and pulse wave analysis (PWA). The National Institute for Clinical Excellence (NICE) determined that patients with office BP>140/90 mm Hg should be evaluated with ambulatory BP monitoring (ABPM) [http://www.nice.org.uk/nicemedia/live/13561/56008/56008.pdf] for diagnosis and monitoring.
Kenneth Connell, MBBS, DM, University of the West Indies, Cave Hill, Barbados, and colleagues at King's College, London, United Kingdom, studied the relationship between office BP and ABPM and the correlation of both BP measures with surrogate markers of disease. The study included 144 healthy volunteers from Barbados assessed with 3 office BP measurements, PWV using a portable physiologic vascular testing unit, and ABPM for 24 hours.
The mean (standard deviation) readings for office systolic/diastolic BP (mm Hg), respectively, were 121 (12)/76 (9) overall, 121 (12)/76 (9) in blacks, 120 (14)/76 (9) in whites (p=NS). The readings for ABPM systolic and office diastolic BP, respectively, were 122 (12)/73 (12) overall, 125 (13)/73 (14) in blacks, and 119 (9)/73 (7) in whites (p=0.004 for ABPM systolic; p=NS for ABPM diastolic). PWV (ms−1) was 10.0 (1.6) overall, 10.1 (1.8) in blacks, and 9.9 (1.3) in whites (p=NS).
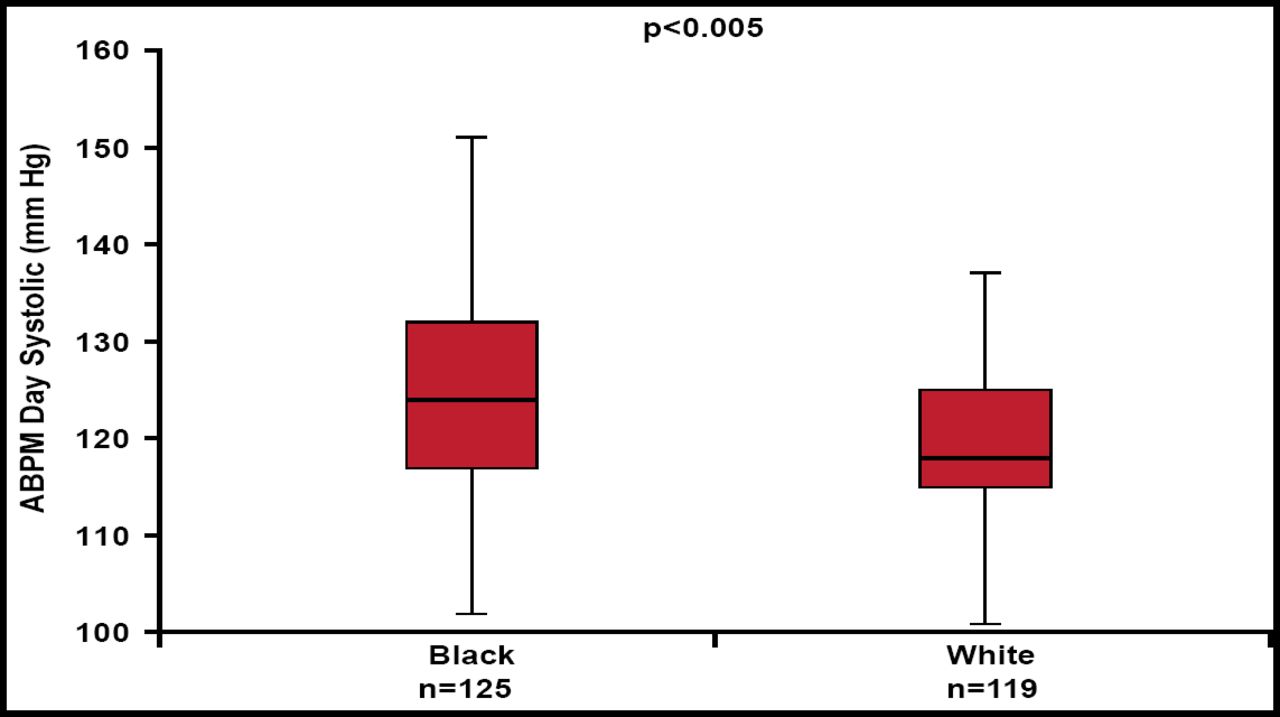
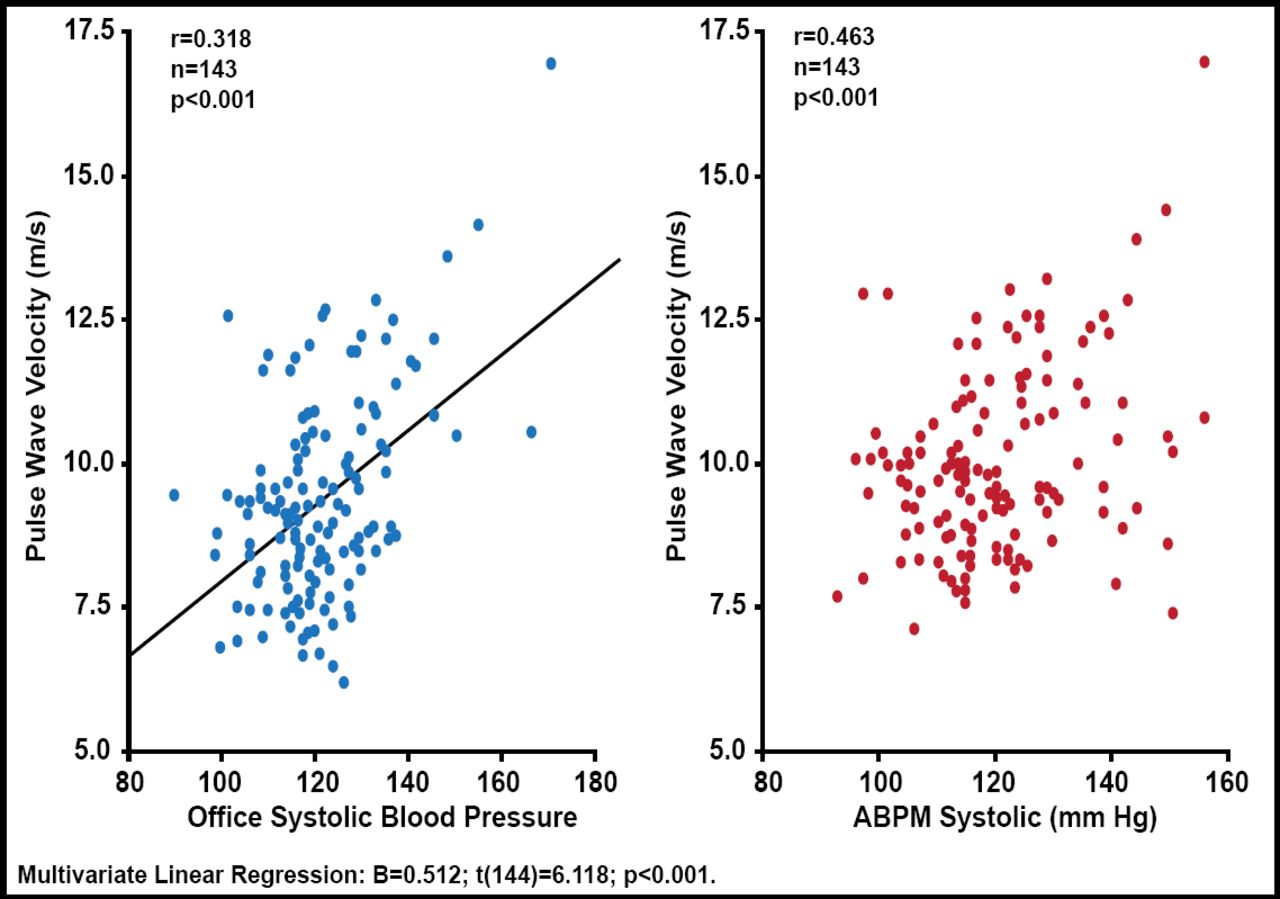
The correlation coefficient for ABPM versus office systolic pressure was r=0.633 (p<0.0001). An ethnic difference in ABPM day systolic BP was observed between black (125 mm Hg) and white subjects (119 mm Hg; p<0.005; Figure 1). The correlation coefficient for PWV versus office systolic BP was r=0.318 (n=143; p<0.001; Figure 2). The correlation coefficient for PWV versus ABPM systolic BP was r=0.463 (n=143; p<0.001).
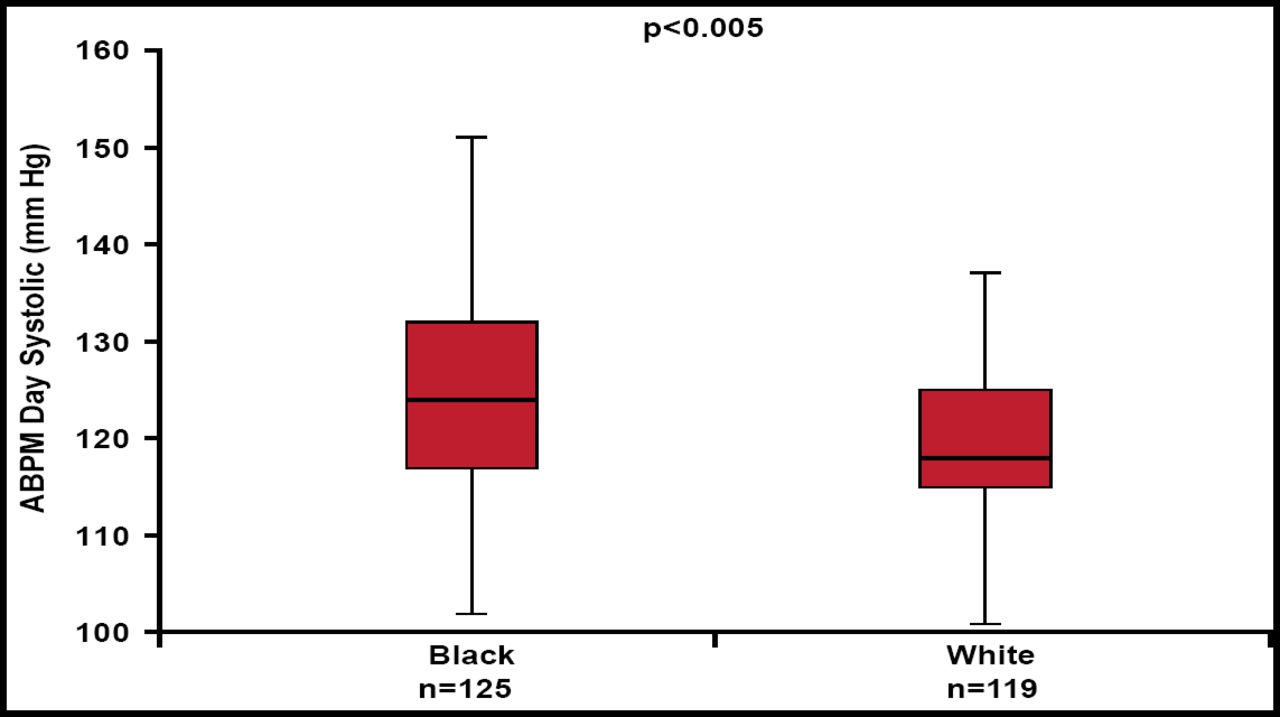
Ethnic Difference in ABPM.
ABPM=ambulatory blood pressure monitoring.
Reproduced with permission from K. Connell, MD.
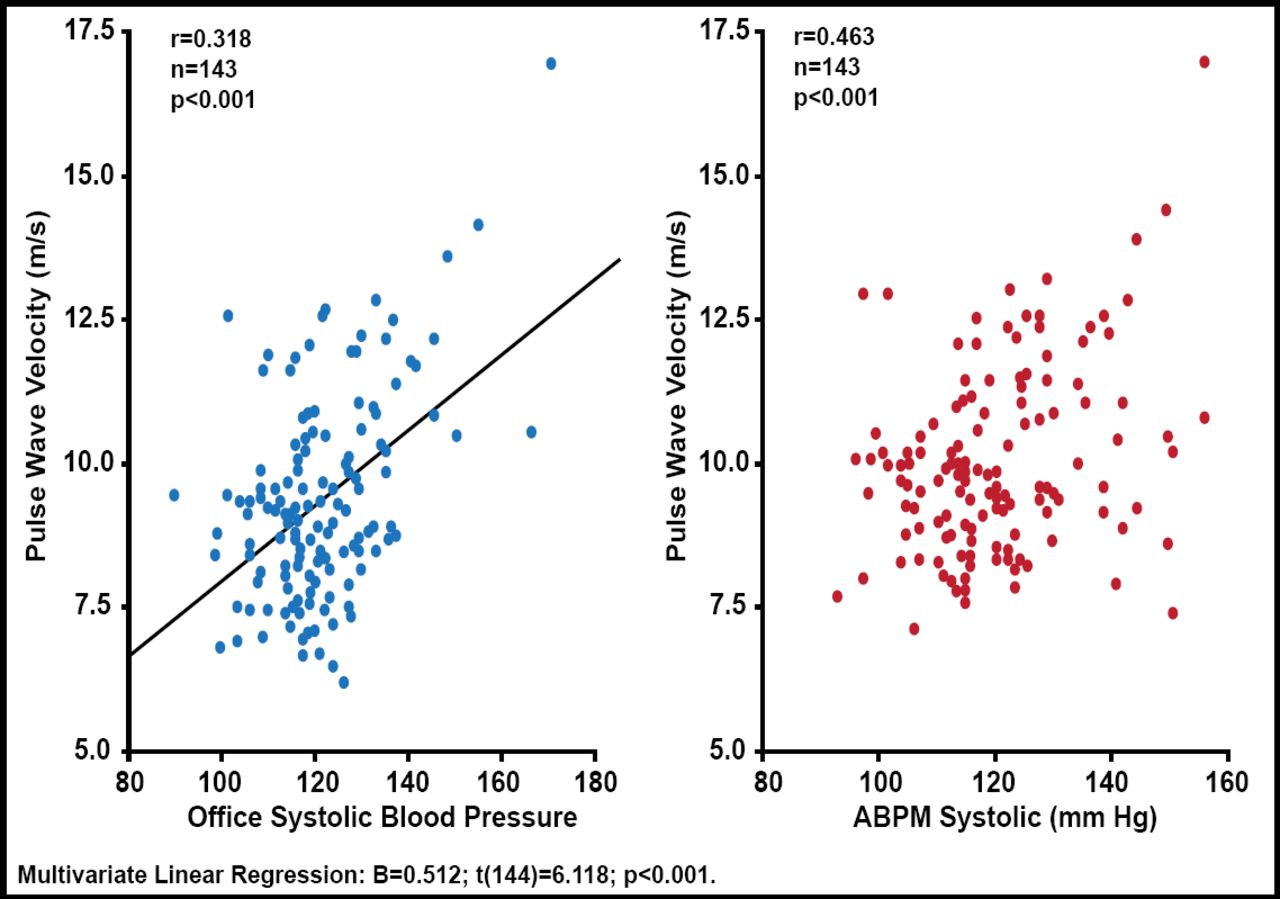
PWV Correlation with Office BP and ABPM.
ABPM=ambulatory blood pressure monitoring; PWV=pulse wave velocity.
Reproduced with permission from K. Connell, MD.
Dr. Connell concluded that there is a significant correlation between office BP and ABPM readings among healthy volunteers in an outpatient practice setting in country. Ethnic differences have been observed in systolic BP on ABPM, with no difference observed with office BP for the same population. Office BP was the strongest predictor of PWV, a marker of arterial stiffness. The NICE guidelines suggest a paradigm shift for the diagnosis of hypertension using ABPM. However, ABPM costs between US $100 and $150, and Dr. Connell wondered whether this is affordable. He suggested that office BP measurements might be just as good or a better predictor than ABPM of surrogate vascular markers.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.