

Summary
The dual pandemics of obesity and diabetes threaten to overwhelm the health systems of countries the world over. What can we do about abdominal obesity? This article addresses challenges and options for dealing with abdominal obesity-related conditions.
- Obesity
- Diabetes Mellitus
- Cardiometabolic Disorder
The dual pandemics of obesity and diabetes threaten to overwhelm the health systems of countries the world over. What can we do about abdominal obesity? Luc Van Gaal, MD, PhD, Antwerp University Hospital, Antwerp, Belgium, addressed challenges and options for dealing with abdominal obesity-related conditions.
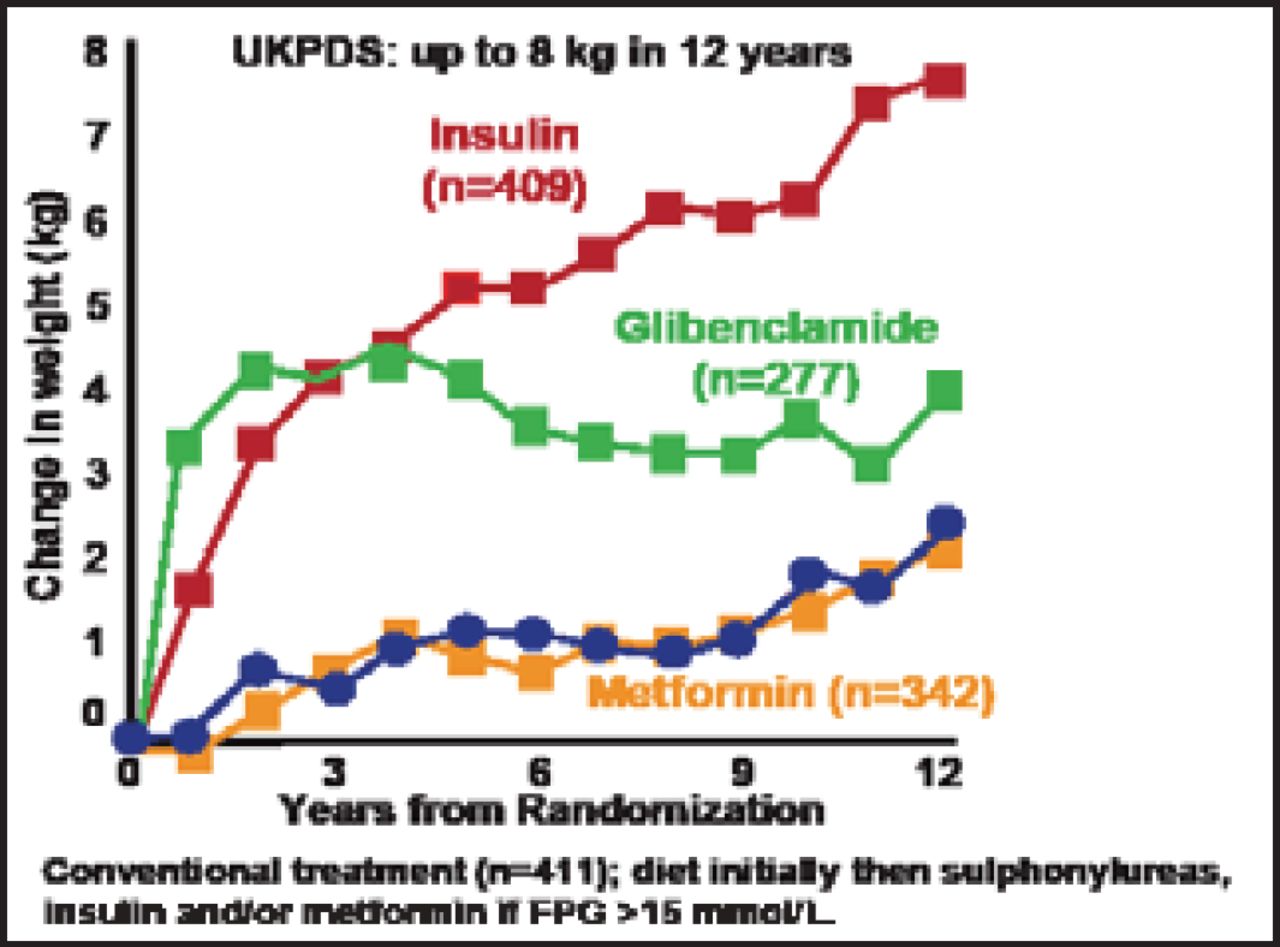
Conventional antidiabetes therapies often increase weight (Figure 1) [UK Prospective Diabetes Study 34. Lancet 1998; Kahn SE et al. N Engl J Med 2006]. A cross-sectional evaluation of participants with type 2 diabetes in the Look AHEAD trial showed that adipose tissue distribution is significantly altered in these patients [Gallagher D et al. Am J Clin Nutr 2009].

Weight Increase With Conventional Approaches for the Treatment of Type 2 Diabetes.
Reprinted from The Lancet, Vol 351/9112, Kahn H et al., Prenatal exposure to famine and health in later life, 1360–1, Copyright (1998), with permission from Elsevier.
According to Prof. Van Gaal, 3 key actions to address this problem include 1) assess risk (ie, visceral fat and comorbid conditions), 2) initiate interventions to reduce total and visceral fat, such as lifestyle changes, pharmacotherapy, and weight loss surgery, and 3) institute preventive measures.
In a recent meta-analysis, Ismail et al. [Obes Rev 2012] assessed the efficacy of exercise interventions on visceral adipose tissue (VAT) content and volume in overweight and obese adults. Data suggested that aerobic exercise in this population is central for exercise programs aimed at reducing VAT. Albu et al [Diabetes 2010] found that changes in overall weight (adipose tissue mass) and hepatic fat were the most important determinants of metabolic improvements.
Pharmacotherapy includes central-acting drugs (eg, sibutramine and topiramate/phentermine combination); lipase inhibition (ie, orlistat); and glucose-lowering drugs. In 1998, Van Gaal et al. [Int J Obes Relat Metab Disord 1998] reported that sibutramine produced statistically and clinically significant decreases in waist circumference and waist-to-hip ratio, and preferentially reduced visceral fat levels. Last year, Gadde et al. [Lancet 2011] found significant improvements in comorbid conditions with a topiramate/phentermine combination.
New and future drugs that target intra-abdominal fat include second-generation peripheral cannabinoid 1 antagonists, 11 β hydroxysteroid dehydrogenase inhibitor, glucagon-like peptide (GLP)-1 analogs/mimetics, sodium glucose cotransporter (SGLT)-2 inhibitors, and leptin-pramlintide combination.
In an investigation of the effects of GLP-1 analog liraglutide, Inoue et al. [Cardiovasc Diabetol 2011] found that liraglutide significantly reduced estimated visceral fat compared with no significant change before medication induction (p<0.005). A study on dapagliflozin, a SGLT-2 inhibitor, showed a decrease in total body weight at Week 24, predominantly by reducing fat mass, VAT, and subcutaneous adipose tissue in patients with type 2 diabetes inadequately controlled by metformin [Bolinder J et al. J Clin Endocrinol Metab 2012].
Resolution of type 2 diabetes is known to be an additional benefit of surgical treatment for severe obesity [Pories WJ et al. Ann Surg 1995], with glycemic control often occurring long before significant weight loss [Mingrone G et al. Diabetologia 1997]. Buchwald et al. [JAMA 2004] reported 98.9% resolution of diabetes with the biliopancreatic diversion or duodenal switch technique and 83.7% for gastric bypass. Data from a subanalysis of the European Hepatic and Adipose Tissue and Functions in the Metabolic Syndrome project found decreases of 25.4±5.9% in weight (kg) and 50±8% in VAT (cm) after bariatric surgery (Table 1) [Van Gaal LJ et al. Subanalysis of EU HEPADIP Project].
Visceral Fat Loss After Weight-Loss Surgery.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.