

Summary
Visceral adiposity is an important correlate of cardiometabolic risk, yet its association after the diagnosis of type 2 diabetes remains unclear [Smith JD et al. J Clin Endocrinol Metab 2012]. This article discusses the association between visceral adiposity, fatty liver, and cardiometabolic risk, and presents results from the International Study of Prediction of Intra-Abdominal Adiposity and Its Relationships with Cardiometabolic Risk/Intra-Abdominal Adiposity [INSPIRE ME IAA; Smith JD et al. J Clin Endocrinol Metab 2012].
- Cardiometabolic Disorder
- Obesity
- Diabetes Mellitus
Visceral adiposity is an important correlate of cardiometabolic risk, yet its association after the diagnosis of type 2 diabetes remains unclear [Smith JD et al. J Clin Endocrinol Metab 2012]. Jean-Pierre Després, PhD, Université Laval, Québec City, Québec, Canada, discussed the association between visceral adiposity, fatty liver, and cardiometabolic risk, and presented results from the International Study of Prediction of Intra-Abdominal Adiposity and Its Relationships with Cardiometabolic Risk/Intra-Abdominal Adiposity [INSPIRE ME IAA; Smith JD et al. J Clin Endocrinol Metab 2012].
INSPIRE ME IAA, a computed-tomography (CT) imaging study, addressed a lack of international data on the contribution of excess visceral adiposity and liver fat to the cardiometabolic risk profile of patients with impaired glucose homeostasis, type 2 diabetes, or cardiovascular (CVD) disease.
The aims of the study were to cross-sectionally determine the history of ischemic CV events and type 2 diabetes and to determine the relationship between visceral adiposity and cardiometabolic risk markers/factors, including waist circumference. As the study included a 3-year follow-up, investigators also studied the relationship between visceral adiposity and the incidence of ischemic CV events and type 2 diabetes over the planned 3-year follow-up period. The primary objective was to assess the independent and combined associations of visceral adiposity and type 2 diabetes to cardiometabolic risk.
The multinational study involved 4277 patients (52% male). Their mean age was 57 years; 60% had hypertension; 39% had type 2 diabetes (fasting glucose ≥7 mmol/L or glucose ≥11.1mmol/L 120') or treatment for diabetes or history of diabetes; 62% had metabolic syndrome (American Heart Association/National Heart, Lung, and Blood Institute); 24% had CVD. Patients were categorized according to visceral adiposity tertiles, type 2 diabetes status, and sex. All results were adjusted for age, body mass index (BMI), geographic region, and physician's specialty.
CT scans were performed at the L4-L5 vertebrae level for abdominal adipose tissue and at the Th12-L1 level for liver attenuation (a marker of liver fat content) between 1 and 3 weeks after the baseline visit [Shores NJ, et al. Dig Dis Sci 2011].
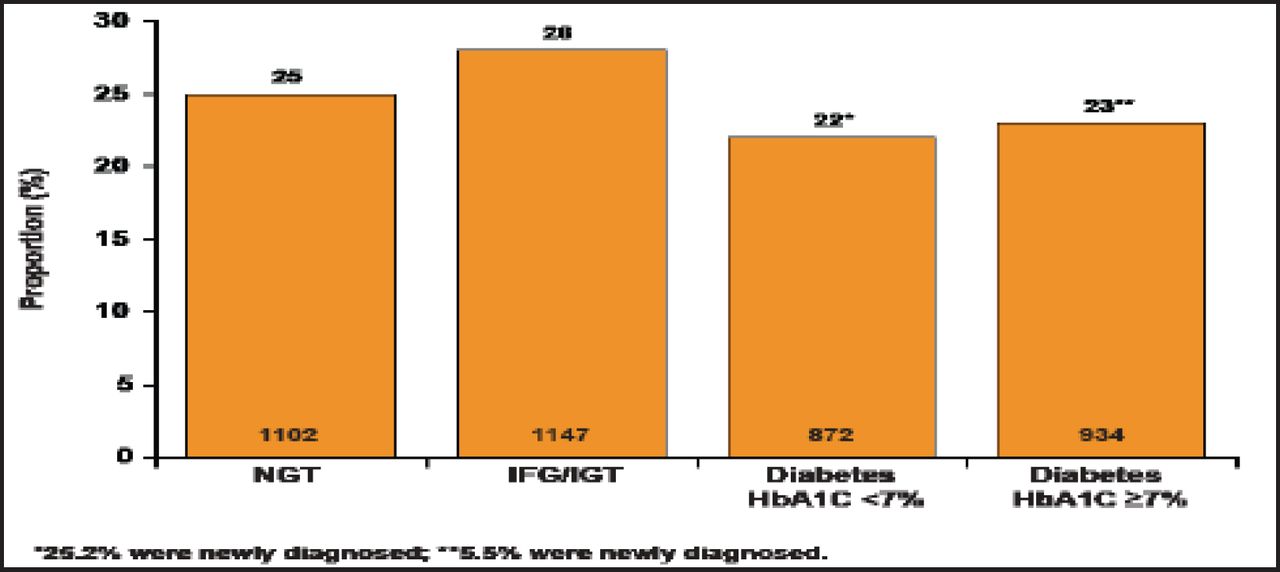
Patients were categorized as having type 2 diabetes if their fasting plasma glucose was at least 126 mg/dL, their 120-min post-75-g oral glucose tolerance test (OGTT) glucose was at least 200 mg/dL, they used antidiabetes medication, and/or had a previous diagnosis of type 2 diabetes [Smith JD et al. J Clin Endocrinol Metab 2012]. Figure 1 shows the proportion of subjects according to glucose tolerance standards [Després JP et al. EASD 2010].

Proportion of Subjects According to Glucose Tolerance Status.
Reproduced with permission from JP Deprés, PhD.
Outcomes showed that higher levels of visceral adipose tissue (VAT) are associated with increased levels of cardiometabolic risk factors, including a more deleterious plasma/lipoprotein profile with higher apolipoprotein (Apo) B and triglycerides and lower high-density lipoprotein-cholesterol in men and women, and lower ApoA1 in women only. Plasma glucose, insulin (fasting and after OGTT), and HbA1C levels were significantly higher with increasing VAT in men and women, and all indices of plasma glucose/insulin homeostasis were higher in men and women with type 2 diabetes.
The prevalence of CVD increased with increasing levels of VAT. Higher levels of VAT were associated with greater prevalence of several clinical CV manifestations in individuals with and without type 2 diabetes (Figure 2). Type 2 diabetes status was positively associated with the presence of CVD in women (p=0.008) but had no effect in men (p=0.5).

Frequency of Prevalent CV Disease in Men and Women Without and with Type 2 Diabetes.
Reproduced with permission from JP Deprés, PhD.
Data indicated that VAT is associated with type 2 diabetes independent of BMI. Adjustment of each parameter separately for age, geographical region, BMI, and recruiting physician's specialty yielded a positive association between waist circumference, systolic blood pressure, triglycerides, and VAT with type 2 diabetes in both men and women.
Based on these outcomes, the researchers concluded that excess visceral adiposity/fatty liver is a key correlate of metabolic abnormalities in patients with and without type 2 diabetes. According to Prof. Després, although waist circumference and BMI are strongly correlated, yet for a given BMI unit, there is substantial individual variation in waist circumference. He noted that waist circumference should not replace but complement BMI in risk assessment [Després JP. J Am Coll Cardiol 2011].
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.