

Summary
Children with diabetes are at high risk for premature cardiovascular disease (CVD), which can lead to mortality later in life. Screening and treatment of modifiable risk factors in young patients with diabetes are important to decrease lifetime risk for CVD. This article discusses several noninvasive surrogate measures that would allow for the stratification of CVD risk, and he presented evidence for more aggressive treatment of patients at the highest risk for macrovascular disease in adulthood.
- Hypertensive Disease
- Diabetes Mellitus
- Prevention & Screening
Children with diabetes are at high risk for premature cardiovascular disease (CVD), which can lead to mortality later in life. Screening and treatment of modifiable risk factors in young patients with diabetes are important to decrease lifetime risk for CVD. R. Paul Wadwa, MD, University of Colorado School of Medicine, Aurora, Colorado, USA, discussed several noninvasive surrogate measures that would allow for the stratification of CVD risk, and he presented evidence for more aggressive treatment of patients at the highest risk for macrovascular disease in adulthood.
Endothelial dysfunction is considered an early stage in the pathogenesis of atherosclerosis. Evidence indicates that endothelial dysfunction in children with diabetes may predispose them to the development of early atherosclerosis [Järvisalo MJ et al. Circulation 2004]. The brachial ultrasound technique can be beneficial for detecting impaired flow-mediated dilation. Another tool for measuring endothelial dysfunction is peripheral arterial tonometry. In one study, children with type 1 diabetes had endothelial dysfunction, as evidenced by lower mean reactive hyperemia peripheral artery tonometry scores when compared with children without diabetes [Haller M et al. Pediatr Diabetes 2007].
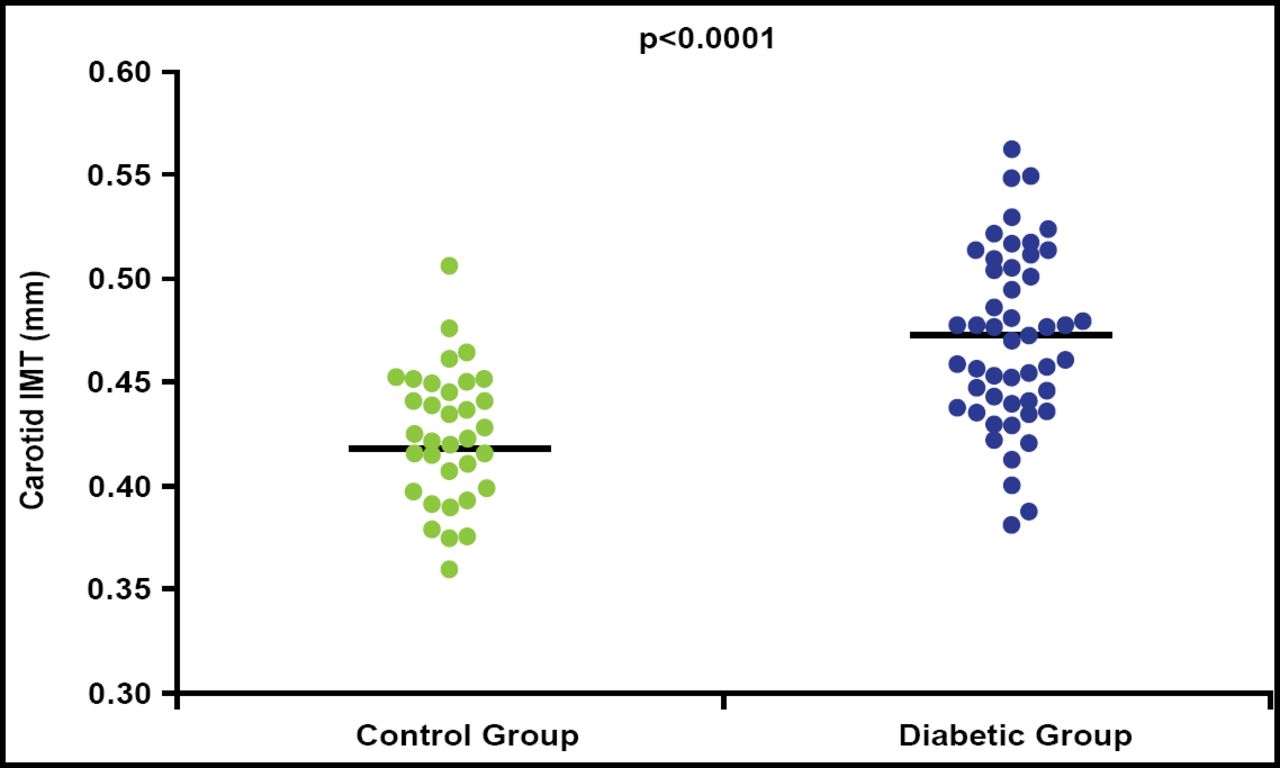
Noninvasive B-mode ultrasonographic measurement of progression of intima-media thickness in the distal common carotid artery is a useful surrogate endpoint for clinical coronary events. Increases in the thickness of the intima and media of the carotid artery are directly associated with an increased risk of myocardial infarction and stroke in older adults without a history of CVD [O'Leary DH et al. N Engl J Med 1999]. Although data are limited in younger patients, one study has shown an increase in carotid intima-media thickness (cIMT) and a decrease in flow-mediated dilation in children (mean age 11 years) with type 1 diabetes (Figure 1) [Järvisalo MJ et al. Circulation 2004]. Preliminary data presented at the 2011 meeting of the American Diabetes Association indicate significantly thicker cIMT in the common and internal carotid in youth with type 1 diabetes compared with controls [Urbina EM et al. Diabetes 2011].

cIMT in Controls and Type 1 Diabetes.
Reproduced with permission from P Wadwa, MD.
In an ancillary study to the SEARCH for Diabetes in Youth study, the measurement of arterial stiffness by pulse-wave velocity, pulse-wave analysis, and brachial artery distensibility indicated that youths with type 2 diabetes had worse arterial stiffness than youths with type 1 diabetes [Wadwa RP et al. Diabetes Care 2010]. Further, pulse-wave velocity was higher than controls in youths with type 1 diabetes with a mean age of 19 years but not in youths with a mean age of 15 years, suggesting that the right time for aggressive intervention to prevent vascular damage would be between the ages of 15 to 19 years [Wadwa RP et al. Diabetes 2011 (two ADA abstracts)].
Coronary artery calcification correlates with overall coronary plaque burden and can be predictive of future coronary events. Although data in adults with diabetes are strong, coronary artery calcification may be of lesser interest in pediatric patients, as there is a relatively low presence of coronary artery calcification in patients aged <30 years [Starkman HS. Diabetes Care 2003].
Echocardiography has been used to document cardiac dysfunction in adults with diabetes. Recent studies have shown that it can detect diastolic dysfunction, increased ventricular septal thickness, and lower circumferential strain compared with nondiabetic controls [Nadeau K et al. J Clin Endocrinol Metab 2010; Salem et al. Pediatr Diabetes 2009]. Further work is needed to evaluate risk factors associated with changes in cardiac structure and function.
Most of these techniques are affordable, available, and safe. Currently, however, they are used in clinical research only. Further work is needed to standardize techniques and the development of normative data that account for changes with age and pubertal development. The results need to be reproducible, and their use should be cost-effective and lead to effective treatment/interventions.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.