

Summary
The recent Apixaban Compared with Warfarin in Patients with Atrial Fibrillation and Prior Stroke or Transient Ischemic Attack trial [Granger CB et al. N Engl J Med 2011; ARISTOTLE; NCT00412984] found apixaban to be superior to warfarin for stroke prevention in a wide range of atrial fibrillation (AF) patients, with significantly lower bleeding risk and lower risk of all-cause mortality [Littrell R, Flaker G. Expert Rev Cardiovasc Ther 2012]. This article results of a comparison of apixaban with warfarin in patients with AF and prior stroke or transient ischemic attack.
- Featured Meeting - Specialty page
- Extrapyramidal & Movement Disorders Clinical Trials
- Cerebrovascular Disease
- Arrhythmias
The recent Apixaban Compared with Warfarin in Patients with Atrial Fibrillation and Prior Stroke or Transient Ischemic Attack trial [Granger CB et al. N Engl J Med 2011; ARISTOTLE; NCT00412984] found apixaban to be superior to warfarin for stroke prevention in a wide range of atrial fibrillation (AF) patients, with significantly lower bleeding risk and lower risk of all-cause mortality [Littrell R, Flaker G. Expert Rev Cardiovasc Ther 2012]. J. Donald Easton, MD, FAHA, University of California, San Francisco, California, USA, presented results of a comparison of apixaban with warfarin in patients with AF and prior stroke or transient ischemic attack (TIA).
ARISTOTLE was a randomized, double-blind, double-dummy trial that included subjects who were aged ≥75 years and had AF and at least one additional risk factor for stroke (previous stroke, TIA, or systemic embolism [SE]; symptomatic heart failure within the previous 3 months or left ventricular ejection fraction ≤40%; diabetes mellitus; or hypertension requiring pharmacologic treatment). A total of 18,201 patients were randomized to apixaban 5 mg oral BID or warfarin (target INR 2 to 3). The primary outcome was ischemic or hemorrhagic stroke or SE. The trial was designed to test for noninferiority, with key secondary objectives of testing for superiority with respect to the primary outcome and to the rates of major bleeding and death from any cause.
The primary objective of the stroke substudy was to determine whether apixaban, as compared with warfarin, had the same advantages in patients with prior stroke or TIA (n=3436) as in all patients (n=14,765) with AF in the ARISTOTLE trial. The primary efficacy outcome was ischemic or hemorrhagic stroke or SE. The primary safety outcome was major bleeding according to the International Society of Thrombosis and Hemostasis (ISTH) definition.
The demographic and clinical characteristics of the Prior Stroke/TIA patients compared with the No Prior Stroke/TIA patients were essentially the same, with 19.5% of the 18,201 ARISTOTLE patients having had a prior stroke or TIA. The only important difference was in the CHADS2 score (mean, SD): 3.7 (0.9) for the Prior Stroke/TIA group versus 1.7 (0.8) for the No Prior Stroke/TIA group. Only 15% of the No Prior Stroke/TIA group had a CHADS2 score that high.
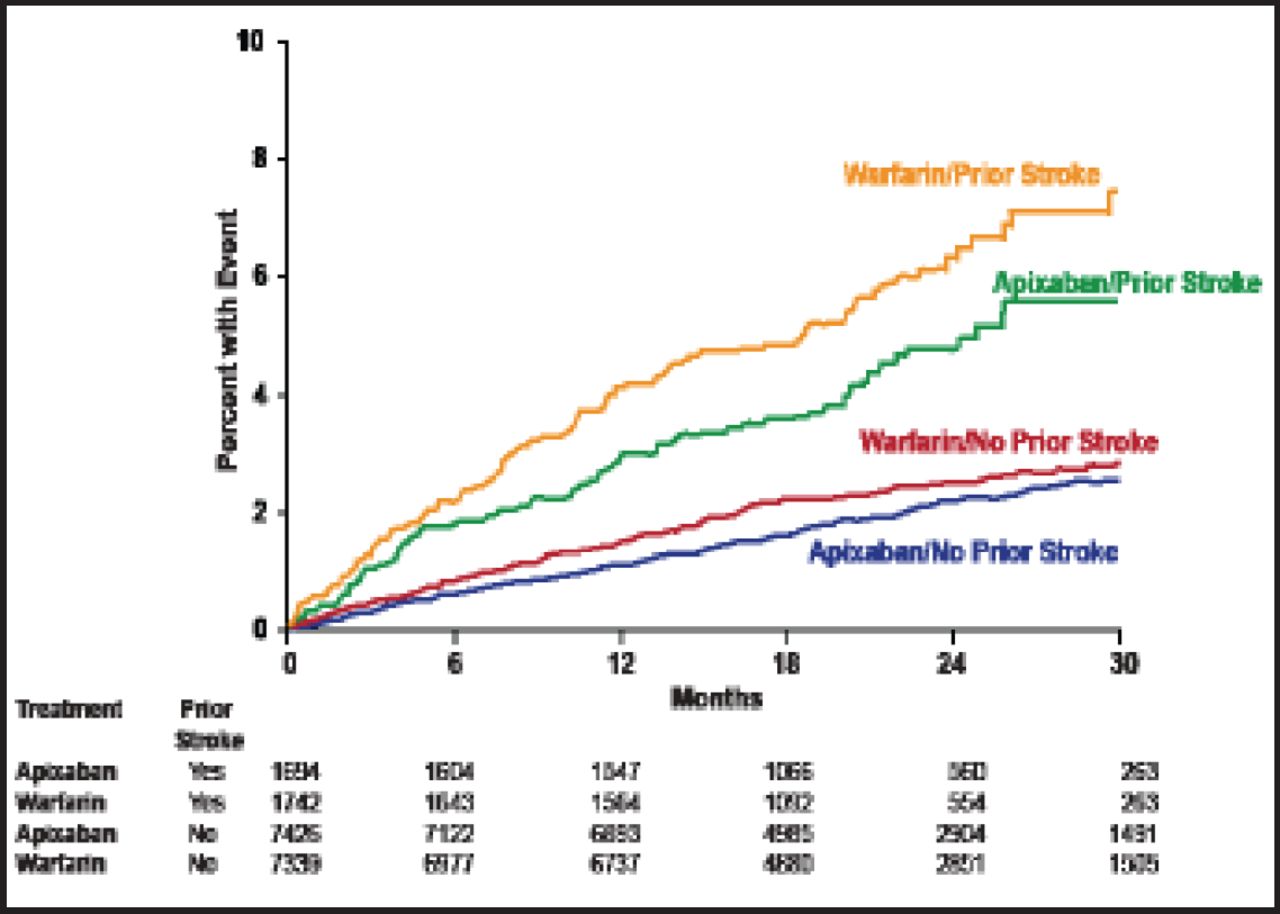
The primary outcome data (Figure 1) showed a considerably higher event rate in the warfarin/Prior Stroke group compared with the apixaban/Prior Stroke group, indicating a greater absolute benefit in the apixaban group. In the hazard ratio outcomes, all p values were nonsignificant, demonstrating comparable benefit in the Prior Stroke/TIA and No Prior Stroke/TIA groups. Efficacy outcomes also had nonsignificant interaction p values, indicating a consistent benefit between the two groups (Table 1). The safety outcomes showed that the benefit always accrued to apixaban. Nonsignificant interaction p values indicated that the results in both groups were equally beneficial.
Stroke Substudy Efficacy Outcomes.

Stroke Substudy Primary Outcome.
Reproduced with permission from JD Easton, MD.
Summary data showed that treatment with apixaban compared with warfarin in patients with AF and prior stroke or TIA reduced stroke and SE by 24%, major bleeding by 27%, intracranial bleeding by 63%, and mortality by 11%.
Overall, the trial demonstrated that in patients with AF and prior stroke or TIA, apixaban is superior to warfarin in preventing stroke or SE; causes less bleeding, especially intracranial bleeding; and results in lower mortality. These outcomes are consistent with those of the main ARISTOTLE trial.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.