

Summary
Acute coronary syndrome (ACS), which encompasses ST elevation myocardial infarction, non-ST elevation myocardial infarction, and unstable angina, is a dynamic event whose pathophysiology should dictate therapy. This article discusses approaches to treatment of ACS.
- Thrombotic Disorders
- Coronary Artery Disease
- Myocardial Infarction
Acute coronary syndrome (ACS), which encompasses ST elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), and unstable angina (UA), is a dynamic event whose pathophysiology should dictate therapy. Victor Elliott, MD, University Hospital of the West Indies, Kingston, Jamaica, discussed approaches to treatment of ACS.
ACS is almost always associated with rupture of an atherosclerotic plaque and partial/complete thrombosis of the infarct-related artery. The identification and definition of the concept of the vulnerable plaque in 2003 contributed to the development of a risk stratification scheme for ACS, in which plaque stability is related to its histological composition (ie, pathological intimal thickening [PIT], thin-capped fibroatheroma [TCFA], thick-capped fibroatheroma [ThCFA], fibrotic plaque, or fibrocalcific plaque) [Naghavi M et al. Circulation 2003]. The dynamic character of plaque was confirmed in a recent study in which virtual histology intravascular ultrasound was used to monitor changes in plaque over a 1-year period. In that study, ∼10% of plaque that was classified as PIT progressed to TCFA compared with 19% to ThCFA, and while 25% of TCFA plaque remained TCFA, ∼60% progressed to ThCFA. Of particular interest was that ∼6% of ThCFA plaque became TCFA [Kubo T et al. J Am Coll Cardiol 2010].
Therapies for unstable ischemic heart disease include medication (eg, antiplatelet agents, anticoagulants, fibrinolytics, and statins) and coronary revascularization with percutaneous coronary intervention (PCI) or coronary bypass surgery (CABG).
Platelets play an important role in atherothrombosis, and platelet activation is implicated in the genesis of ACS. While aspirin has been in clinical use as an antithrombotic for almost a half-century, more potent antiplatelet agents, like clopidogrel, prasugrel, and ticagrelor, which function by interrupting specific sites in the sequence of platelet activation, have become part of routine care for patients with ACS, in addition to aspirin. The TRITON TIMI 38 study showed that prasugrel was superior to clopidogrel in terms of reducing recurrent cardiovascular events in patients with ACS who were undergoing PCI. In an analysis of patients with STEMI in this trial, the primary study endpoint (cardiovascular death, MI, and stroke at 15 months) was reduced from 12.4% for clopidogrel to 10.0% with prasugrel (RRR=21%; p=0.02) [Montalescot et al. ESC 2008]. Similarly, prasugrel was more efficacious than clopidogrel in patients with non-STE ACS (RRR=19%; p<00.001) [Wiviott SD et al. NEJM 2007].
Glycoprotein IIb/IIIA inhibitors interrupt the final step of platelet aggregation. These intravenous agents (abciximab, eptifibatide, and tirofiban) are fast-acting and reversible and are indicated for use in the acute setting, particularly at the time of PCI. They improve vessel patency, reduce reinfarction rates, and decrease mortality. In the PRISM trial, tirofiban significantly reduced the 30-day event rate in medically managed (p=0.004) and revascularized patients (p=0.02) with NSTEMI ACS who had evidence of myocardial necrosis [Heeschen C. et al. Lancet 1999].
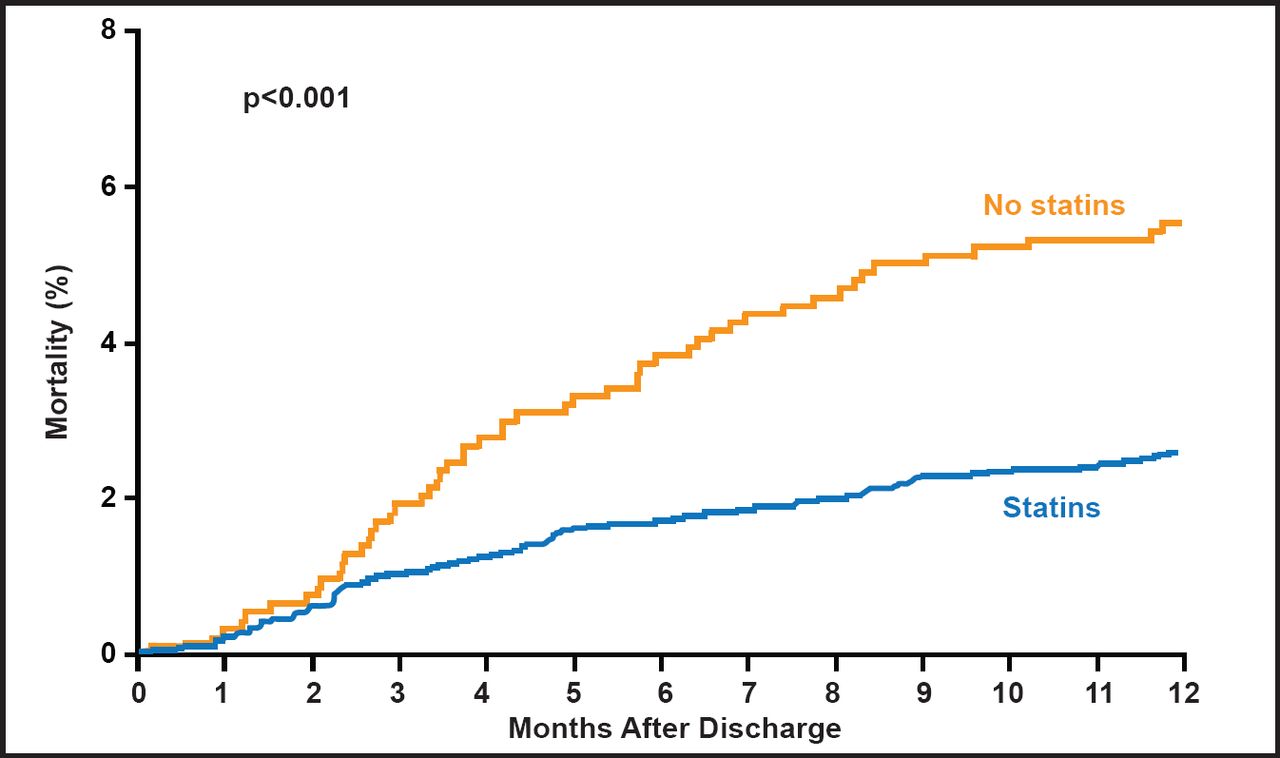
Statins also play an important role in the management of ACS because of their anti-inflammatory effect. The key is to start statins early and use high doses. The REVERSAL study showed that atorvastatin significantly halted atherosclerosis. The ASTEROID study showed that in statin-naïve patients with coronary artery disease, regression of coronary atherosclerosis can be achieved with intensive statin therapy with 40 mg rosuvastatin. In that study, rosuvastatin significantly reduced low-density lipoprotein cholesterol by 53% (p<0.001) and significantly raised high-density lipoprotein cholesterol by 14.7% (p<0.001) [Nissen S et al. JAMA 2006; Ballantyne C et al. Circulation 2008]. Importantly, PROVE IT – TIMI 22 and MIRACL have shown that starting these lipid-lowering drugs immediately after an ACS is associated with a significant reduction in cardiovascular events. Statin therapy after coronary artery stenting is associated with an unadjusted odds ratio (OR) of 0.46 (95% CI, 0.33 to 0.65), indicating a 54% reduction in the risk of death at 1 year (Figure 1) [Schomig A et al. J Am Coll Cardiol 2002].
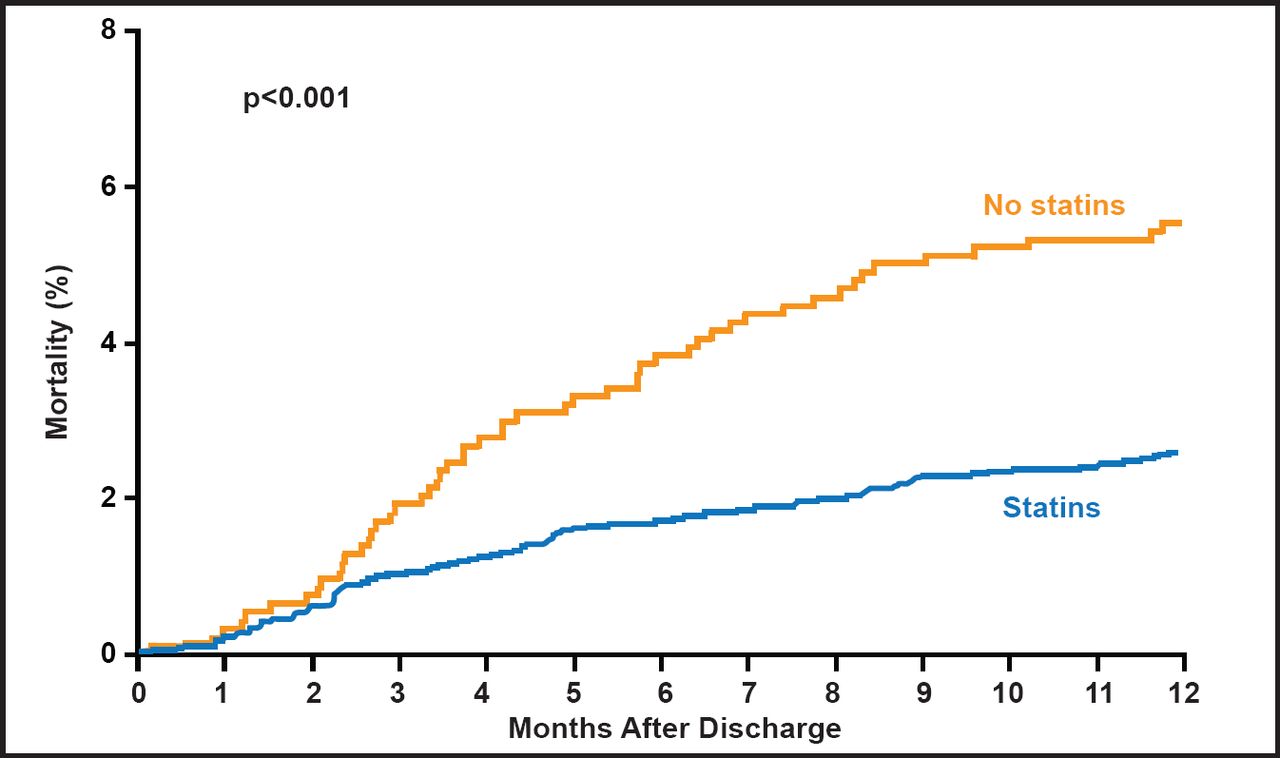
Cumulative One-Year Mortality Curves for Patients with and without Statins.
Reproduced with permission from the American College of Cardiology. Schömig A et al. Statin treatment following coronary artery stenting and one-year survival. J Am Coll Cardiol. Jan 1, 2002;40(5):854–861.
Dr. Elliot stressed the need to begin therapy by initially stabilizing the plaque before it ruptures and following the recommended treatment guidelines.
Myocardial revascularization is a key component in the management of patients with ACS. Outcomes can be optimized by early treatment and risk stratification and by using an adequate antithrombotic regimen before revascularization. Restoring coronary flow, limiting infarct area, preserving left ventricular function, reducing ischemic effects, and limiting thrombus burden are all important goals in treating patients with ACS; however, according to João Morais, MD, Serviço de Cardiologia Hospital de Santo André, EPE Leiria, Portugal, the primary goal should be improving survival. This is best achieved in the acute setting with the use of antithrombotic drugs, followed by PCI (including coronary stenting) or CABG.
The last 30 years has seen a continuous evolution regarding the treatment of STEMI and NSTEMI, beginning with the use of lytic therapy, to mechanical reperfusion and then PCI. With time and experience, the invasive approach to treating NSTEMI has proved to be more efficacious for most patients. Long-term data (out to 5 years) from the FRISC II (Fragmin and Fast Revascularization during Instability in Coronary Artery Disease) study noted that 19.9% of patients who received invasive therapy experienced death or MI compared with 24.5% who received noninvasive therapy (RR, 0.81; 95% CI, 0.69 to 0.95; p=0.009) [Lagerqvist B et al. Lancet 2006]. The TACTICS-TIMI 18 trial results support the use of an early invasive strategy in NSTEMI, high-risk (TIMI risk score 3 to 7) patients with UA and MI who have been previously treated with aspirin, heparin, and the glycoprotein IIb/IIIa inhibitor tirofiban. A more recently published overview of three crucial trials [FRISC-2; ICTUS; RITA-3] confirmed the benefit of early revascularization in higher-risk patients with NSTEMI.
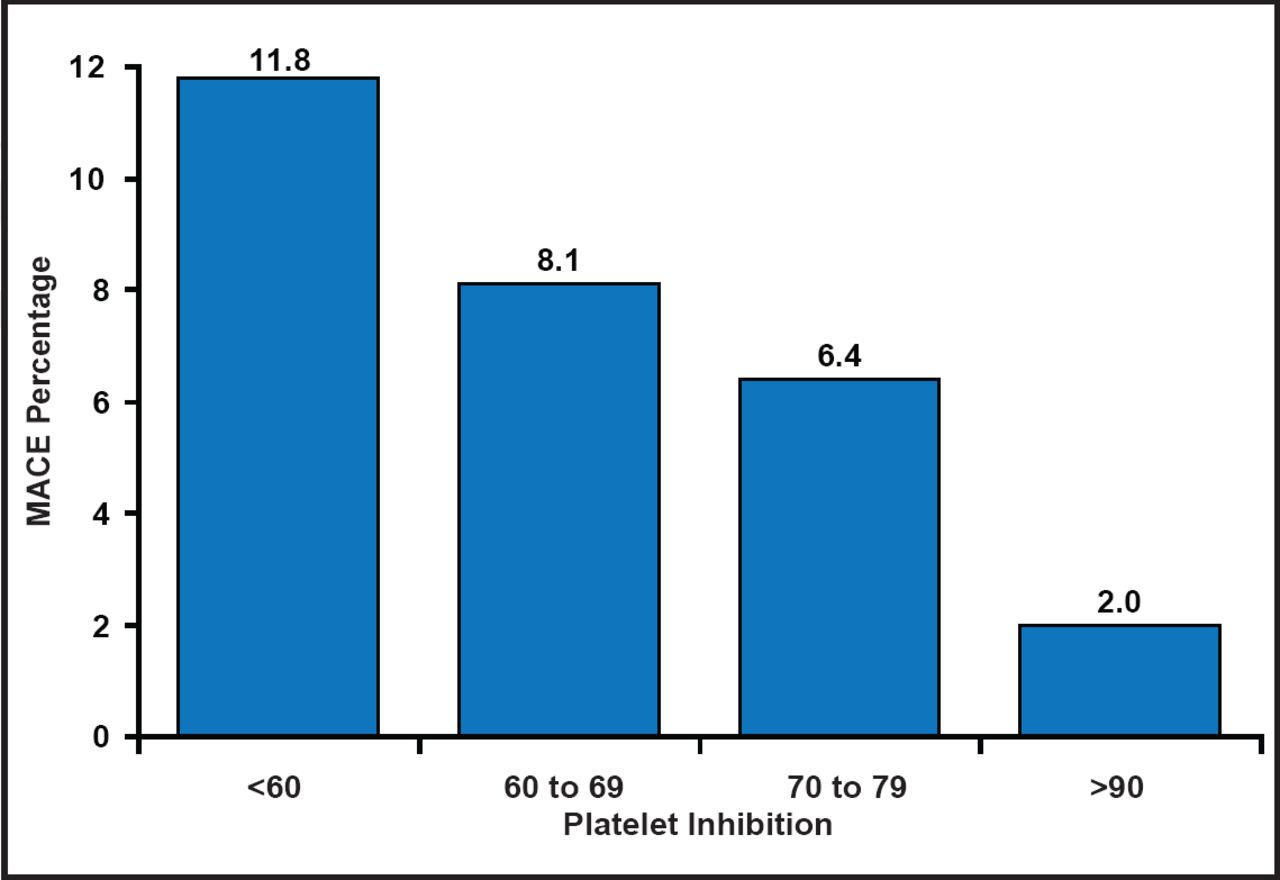
Achieving sufficient platelet inhibition in order to minimize thrombotic complications in patients who are undergoing PCI is a significant part of ACS treatment strategy. The level of platelet inhibition that is achieved has been independently associated with the risk of major adverse coronary events (composite of death, MI, and urgent target vessel revascularization) after PCI (Figure 2) [Steinhubl S et al. Circulation 2001]. The efficacy of the antiplatelet agent clopidogrel (300 mg followed by 75 mg daily), given in addition to aspirin in NSTE-ACS patients through 12 months from their index event, was assessed in the CURE trial. The primary outcome of cardiovascular death, MI, or stroke occurred in 9.3% of the patients in the clopidogrel group and 11.4% of the patients in the placebo group (RR, 0.80; 95% CI, 0.72 to 0.90; p<0.001) [Yusuf S et al. N Engl J Med 2001]. Newer antiplatelet agents, like prasugrel and ticagrelor, are more potent and have a faster onset of action compared with clopidogrel. These agents have been tested against clopidogrel in the TRITON TIMI 38 trial (prasugrel) and the PLATO trial (ticagrelor), with both studies demonstrating superiority in the reduction of recurrent cardiovascular events with the newer-generation ADP receptor blockers.
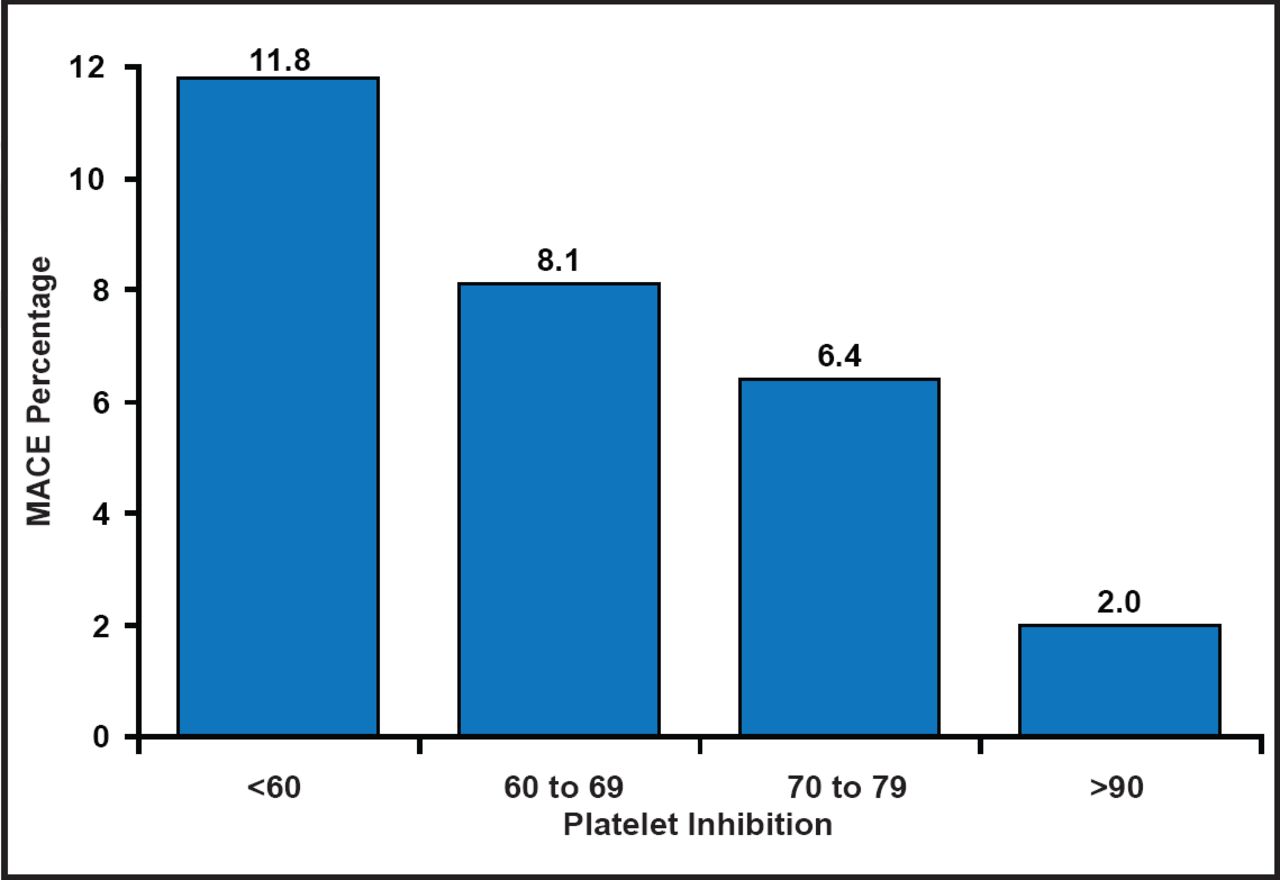
Relationship of Platelet Level Inhibition and MACE.
Reproduced with permission from J. Morais, MD.
Though the best time for intervention is still a matter of debate, in the Timing of Intervention in Acute Coronary Syndromes (TIMACS) trial, slight differences were noted for early intervention (coronary angiography ≤24 hours after randomization) versus delayed intervention (coronary angiography ≥36 hours after randomization). At 6 months, the primary outcome occurred in 9.6% of patients in the early intervention group, as compared with 11.3% in the delayed intervention group (HR, 0.85; 95% CI, 0.68 to 1.06; p=0.15). As previously noted, subgroup analyses showed that early intervention improved the primary outcome in the third of patients who were at highest risk (GRACE score ≥140) but not in the two-thirds at low-to-intermediate risk [Mehta SR et al. N Engl J Med 2009]. Thus, international guidelines recommend an early invasive strategy for NSTEMI patients with high-risk ACS.
Cardiac disease rates in the Caribbean are similar to those in the United States and Europe (Table 1), but there is a two-tiered system of cardiac care (public and private), which impacts treatment availability. Richard Ishmael, MD, Queen Elizabeth Hospital, St. Michael, Barbados, discussed the possibility of meeting the European Society of Cardiology (ESC) guidelines for ACS in the Caribbean, while urging the Caribbean Cardiac Society to compile its own guidelines.
Leading Causes of Death.
Guideline-based treatment of ACS patients with STEMI by primary PCI is possible in the Caribbean but only in private hospitals, and the management is directly related to the individual facility, the cost, and patients' ability to pay. STEMI treatment by fibrinolysis is generally available in most public hospitals in the Caribbean; however, follow-up coronary angiography regarding the need for PCI or CABG is not readily available. Fibrinolytics are widely available in the region, although streptokinase is more commonly used than t-PA, due to a marked difference in cost. Management is limited by the ability to monitor patients adequately due to lack of beds and trained nurses. Dr. Ishmael believes that the best way to treat patients in public hospitals with state-of-the-art care for ACS (STEMI) is to first begin fibrinolysis, followed by transfer to a private facility for coronary angiography and consideration for PCI.
For patients with NSTE-ACS, treatment that is based on the ESC guidelines is attainable both in public and private hospitals. However, in public hospitals in some regions of the Caribbean, blood biomarkers may not be always available for early diagnosis. The resource challenges that are noted above in patients with STEMI also apply to patients with NSTE-ACS, and in addition, follow-up cardiac testing (ie, nuclear stress testing, CT angiography, and coronary angiography) is often not available in public hospitals.
Overall, in the Caribbean, management of ACS is hampered by a critical shortage of cardiac cath lab facilities and skilled cardiologists and nurses. In addition, patients often present late after onset of chest pain, reducing the opportunity for early intervention. “Governments in the region are urged to partner with private institutions to provide the best possible cardiac care for their citizens,” said Dr. Ishmael.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.