

Summary
To effectively address the escalating social and economic costs of diabetes-related morbidity, the onus lies with the epidemiologist to discern the nature of the problem and what is driving this steep rise in global disease incidence.
- Cardiometabolic Disorder
- Nursing
- Diabetes Mellitus
- Prevention & Screening
- Obesity
A highlight of the ADA conference is the lecture that is given by the recipient of the Kelly West Award, an honor that is given annually in recognition of outstanding contributions in the field of diabetes epidemiology. The 2010 award was given to Frank B. Hu, MD, PhD, Harvard School of Public Health, Boston, MA.
“There is no question that we are in the midst of a global epidemic of diabetes,” said Dr. Hu. To effectively address the escalating social and economic costs of diabetes-related morbidity, the onus lies with the epidemiologist to discern the nature of the problem and what is driving this steep rise in global disease incidence.
Dr. Hu first considered the rates of disease incidence by pattern. Globally, three patterns have emerged: the gradual increase in incidence, as seen amongst those of Caucasian ancestry in North America and Europe; the accelerated growth in type 2 diabetes mellitus (T2DM) prevalence that is being observed in Asian, Arab, and Latin American populations; and the dramatic expression of T2DM as seen amongst indigenous populations, such as the Pima Indians of the American Southwest [Bhattarai MD et al. J Nepal Med Assoc 2009].
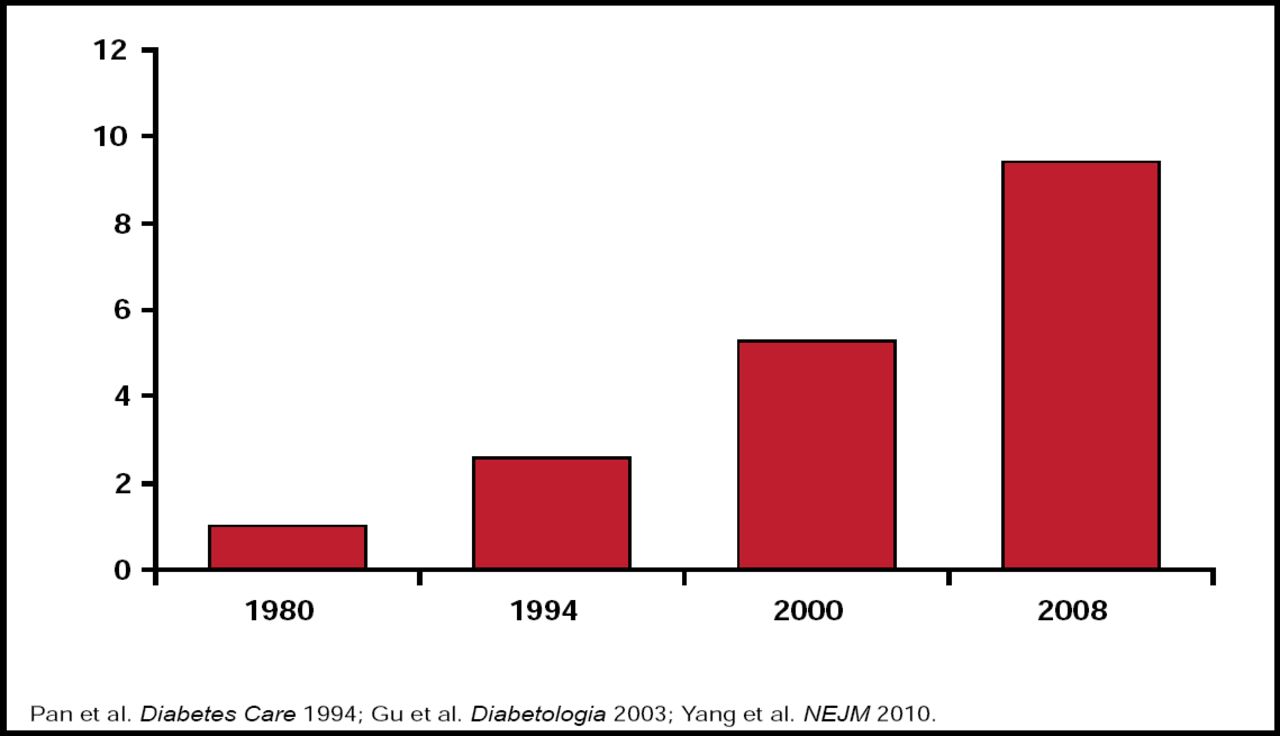
The rapidity of increase in disease incidence in Asia can not be overstated. In China, less than 1% of the population had diabetes in 1980. By 2008 nearly 1 in 10 Chinese adults were considered to have diabetes, with many of these undiagnosed (Figure 1) [Yang W et al. N Engl J Med 2010]. Similar figures describe the problem's scope in India, where the prevalence of diabetes has increased from 2% in 1971 to nearly 20% in 2008 [Ramachandran A et al. Diabetes Care 2008].
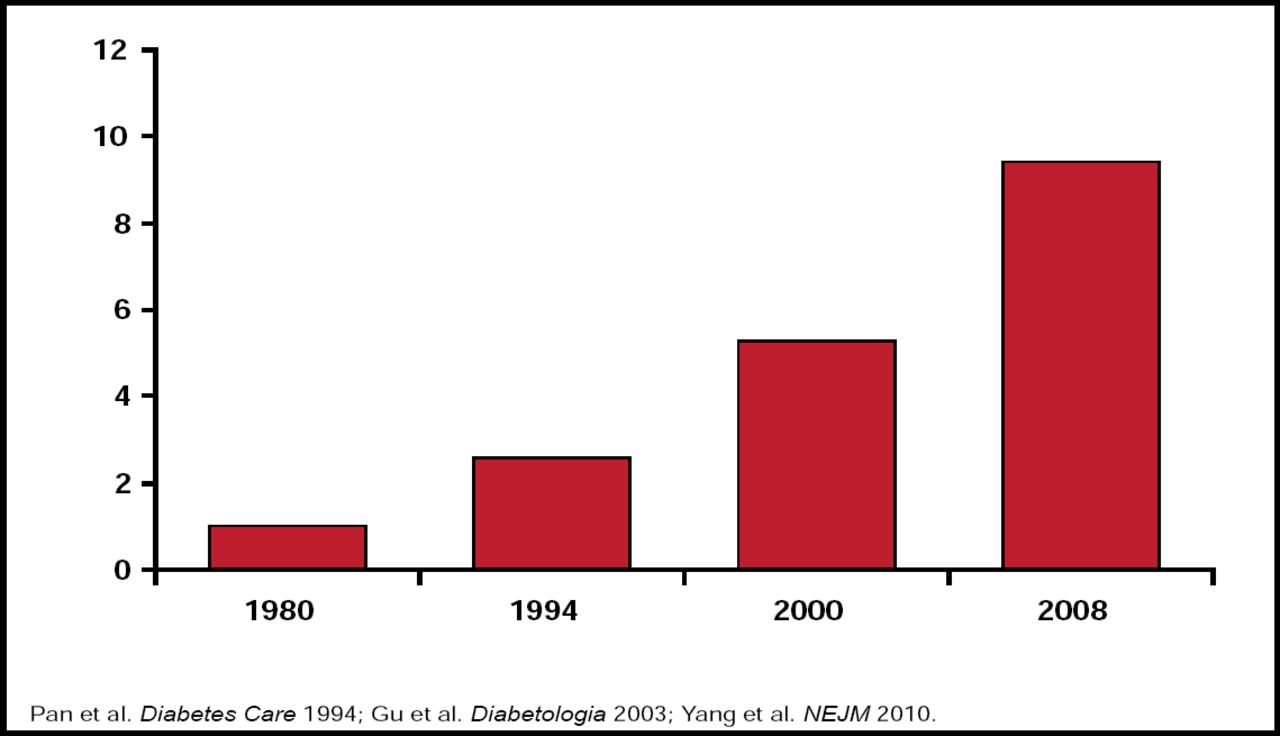
Escalating Diabetes Epidemic in China.
Reproduced with permission from F. Hu, MD, PhD.
Dr. Hu and colleagues established several characteristics of the diabetes epidemic that is specific to Asian populations. The most striking characteristic is that Asians develop the disease at lower values of BMI compared with Caucasians. This is demonstrated by China's much lower rates for obesity compared with the West; yet in the present day, China is demonstrating nearly equivalent rates of diabetes incidence [Chan JC et al. JAMA 2009]. Disease prevalence is expected to worsen, as China is currently undergoing a period of rapid nutritional change and is moving toward a Western diet and lifestyle. In a related dynamic that exacerbates the problem of T2DM, Asian women are predisposed to developing gestational diabetes, thereby placing their children at addition risk for developing T2DM later in life.
The Role of Diet, Lifestyle, and Gene-Environment Interactions in the Global Epidemic of Type 2 Diabetes
Dr. Hu's research has been focused on the large cohorts of the Nurses' Health Study (n=121,700), the Health Professionals Follow-Up Study (n=52,000), and Nurses' Health Study II (n=116,000). Observations from these studies have been ongoing for ∼30 years and have contributed to many fundamental observations that have been related to diabetes epidemiology—not the least of which is the close relationship between BMI and T2DM onset. Further links were established between smoking, as well as alcohol consumption, and the incidence of diabetes. While smoking increased the risk of diabetes in a dose-response fashion, individuals who did not drink at all were at an increased risk compared with those who drank moderately [Rimm et al. BMJ 1995; Wannamethee SG et al. Arch Intern Med 2003].
While the connection between excessive caloric intake, the resulting obesity, and T2DM is well recognized, Dr. Hu asserted that the quality of diet has independent effects on risk. Several dietary determinants of T2DM have been identified. Higher consumption of cereal fiber and polyunsaturated fat is associated with lower risk of diabetes, whereas higher trans fat and glycemic load, a marker of refined carbohydrates, is associated with greater risk. These data speak to the importance of the quality of fat and carbohydrates in determining overall risk. Many developing countries are beginning to move away from whole grain-rich diets to diets with refined carbohydrates [Hu FB et al. N Engl J Med 2001].
Types of carbohydrates have significant influence on the risk of diabetes. Results from a recent meta-analysis show that a 2-increment serving per day of whole grains is associated with a 21% lower risk of developing diabetes [de Munter JS et al. PLoS Medicine 2007]. Conversely, it has been demonstrated that sugar-sweetened beverages (SSBs) are associated not only with weight gain but also with increased risk of T2DM. This relationship remains significant even after adjusting for BMI, suggesting that the adverse impact of SSBs is not entirely mediated through excess weight [Schulze MB et al. JAMA 2004].
Dr. Hu also discussed modern dietary patterns as they relate to the phenomenon of inflammation and diabetes morbidity. Several epidemiological studies demonstrate the association of elevated plasma concentrations of inflammatory cytokines, such as TNF alpha, interleukin-6, and C-reactive protein, and increased risk of diabetes. A dietary pattern that is characterized by higher intake of SSBs, refined grains, processed meats, and margarine and lower intake of wine, coffee, and vegetables is strongly associated with inflammatory cytokine concentrations and risk of T2DM [Schulze MB et al. Am J Clin Nut 2005]. These data provide epidemiological evidence to link overall dietary patterns, inflammation, and diabetes risk, said Dr. Hu.
The Thrifty Genotype Versus Thrifty Phenotype
Returning to the theme of the international/ethnic differences in diabetes risk, Dr. Hu reviewed several potential mechanisms for increased susceptibility to diabetes in Asians. First, Asians tend to exhibit the metabolically obese phenotype of increased central or abdominal obesity despite having a normal BMI. Second, Asians may have an enhanced genetic predisposition to diabetes, due to over-representation of the so-called “thrifty genotype.” Third, exposure to undernutrition in utero, which is common in Asian populations, may have long-term consequences on risk of T2DM and other metabolic diseases in later life. Finally, there might be interactions between genetic predispositions regarding T2DM risk and rapid changes in diet and lifestyle.
Ethnic differences in insulin sensitivity have been consistently demonstrated. Using an euglycemic clamp, one group of investigators found that among age- and BMI-matched young adults, Caucasians have the highest insulin sensitivity, followed by Chinese and South Asians. As measured by homeostasis model assessment of insulin resistance, Southeast Asians and Indians exhibit the highest resistance, whereas Caucasians have the lowest insulin resistance [Dickinson S et al. J Nutr 2002].
The “thrifty genotype,” a hypothesis that was proposed by James Neel, postulates that obesity and T2DM are caused by positive selection of genotypic efficiency in metabolism and energy storage, thereby conferring advantage in times of nutrient scarcity but leading to obesity during a modern age of abundance [Neel JV. Am J Hum Genet 1962; Neel JV. Bull World Health Organ 1999]. This hypothesis, seen in historical perspective, may explain the extraordinary rates of diabetes that have been seen amongst the Pima Indians. However, there is little empirical evidence that the obesity and diabetes genes that have been identified so far are “positively selected.”
Extending the idea of the thrifty genotype to the microenvironment, it is further proposed to explain the observation that exposure to intrauterine undernutrition, a condition that is highly common in rural Asia, leads to fetal phenotype programming of decreased beta-cell function. When subsequently exposed to a Westernized diet in adult life, the risk of diabetes is significantly increased. In a recent study, Dr. Hu and colleagues found that exposure to the Chinese famine (1959–1961) during fetal life was significantly associated with increased risk of hyperglycemia and T2DM in adulthood. This association appears to be exacerbated by a nutrition-rich environment in later life (Li et al. Diabetes 2010 Jul 13. [Epub ahead of print]). This observation is consistent with the “thrifty phenotype” hypothesis.
Is the Die Cast? What Does This Mean?
Given current economic trends, it seems clear that the Eastern hemisphere will increasingly adopt the dietary and lifestyle patterns of the West. In light of a strong “obesogenic” environment, coupled with genetic predisposition for diabetes, the global diabetes epidemic has no sign of abating. However, said Dr. Hu, T2DM is largely preventable through diet and lifestyle modifications. Dr. Hu's work in the Nurses' Health Study cohort supports this assertion, demonstrating that 90% of potential diabetes incidence could be prevented by lifestyle interventions [Hu FB et al. N Engl J Med 2001]. In the China Da Qing study, there was a sustained 40% reduction in risk for the intervention group at 14 years follow-up postintervention (Li G et al. Lancet 2008]. It is remarkable that nearly all of the participants in the control group converted from impaired glucose tolerance to diabetes during the study period. Intervention trials that were conducted in Finland, the US, and India have also demonstrated the benefits of lifestyle intervention for diabetes prevention. As demonstrated by the DPP group, the benefits of lifestyle intervention have the potential to counteract the increased risk that is conferred by the TCF7L2 genotype [Florez JC et al. N Engl J Med 2006].
In closing, Dr. Hu warned that T2DM has become a global public health crisis that threatens the health and economy of all nations and developing countries in particular. The good news is that the majority of T2DM cases can be prevented through diet and lifestyle modification. However, the adoption of a healthy diet and lifestyle requires not only individual behavioral changes but also changes in our food and social environments.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.