

Summary
Guidelines for the management of hypertension (HT), aiming at providing the most balanced recommendations that are supported by evidence-based approaches, are currently in place and focus on mean blood pressure (BP) values. However, questions have been raised as to whether or not other models or algorithms are more suitable for HT assessment and treatment. This article discusses the issue of BP variability and guidelines from a practical perspective.
- Cardiology Guidelines
- Hypertensive Disease
Guidelines for the management of hypertension (HT), aiming at providing the most balanced recommendations that are supported by evidence-based approaches, are currently in place and focus on mean blood pressure (BP) values. However, questions have been raised as to whether or not other models or algorithms are more suitable for HT assessment and treatment. Anthony M. Heagerty, MD, University of Manchester, Manchester, UK, discussed the issue of BP variability and guidelines from a practical perspective.
ESH/ESC 2007 guidelines recommend a variety of treatment approaches, depending upon mean BP (ranging from normal to high normal and Grades 1 through 3 HT) and the type and number of other risk factors that are present [ESH/ESC Task Force on the Management of Arterial Hypertension. J Hypertens 2007]. According to a study by Rothwell and colleagues, visit-to-visit variability in sytolic BP and maximum systolic BP is a strong predictor of stroke and other cardiovascular (CV) events, independent of mean BP. Additionally, this variability accounted for a difference in treatment effect that was observed in two large trials (UKTIA and ASCOT) [Rothwell PM et al. Lancet 2010]. This stroke risk may be reduced with a reduction in visit-to-visit BP variability by initiating calcium channel blocker and diuretic therapy. β-blocker therapy appeared to be the least effective for the reduction of visit-to-visit variability and associated stroke risk (Figure 1) [Rothwell PM et al. Lancet Neurology 2010].

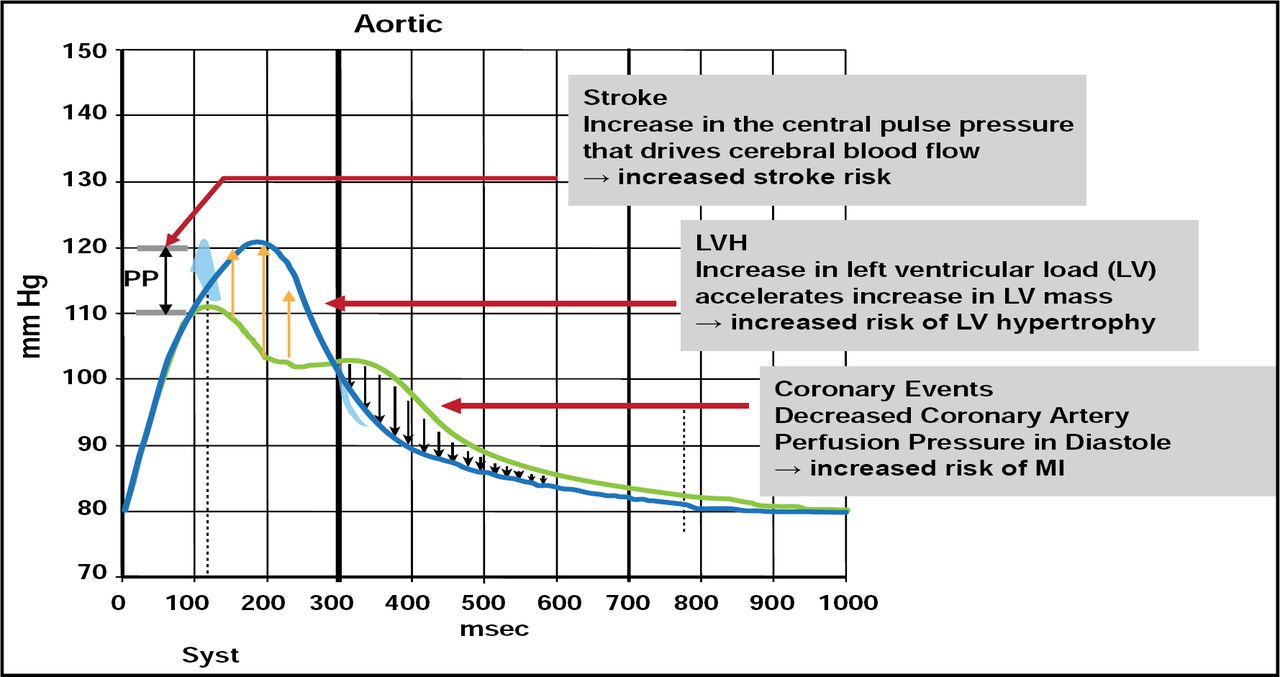
Role of Increase in Central Aortic and Pulse Pressure in the Increase of CV Events.
Reproduced with permission from A. Heagerty, MD.
These new data regarding BP variability provide useful information about risk assessment and may be helpful when considering treatment strategies in the future. However, more research is needed to determine the clinical utility of this measurement. Assessment of BP variability is required in everyday practice, but quantifying such instability in this setting poses a challenge. While we now know that stable BP is better than episodic HT, a clinically translatable test that utilizes these data has yet to be developed. Additionally, treatment algorithms should confirm a downgrade of β-blockers and calcium channel blockers as first-line therapy for all age groups.
Prof. Heagerty explained the role of visit-to-visit BP variability in guideline improvement and treatment optimization. Ambulatory BP monitoring may be too narrow a focus and may not identify those at highest risk. Emphasis should be on consistency of BP control and stabilization in order to properly assess risk and manage HT. The incorporation of visit-to-visit variability into treatment guidelines will provide more accurate risk prediction and will broaden the focus of new drug development to include BP-stabilizing medications, which may be better suited to prevent stroke than currently recommended approaches.
Though current guidelines are useful for determining an appropriate treatment strategy for a variety of hypertensive patients, there appear to be gaps in these recommendations that are related to BP variability and associated risk. Further prognostic studies are warranted before BP variability can be incorporated into guidelines and clinical practice. A quantitative assessment algorithm is also needed to ensure that the BP variability treatment approaches are reliable and accurate for future widespread use. Recent data regarding this aspect of HT are promising, but it would be premature to alter strategies at this time, based on the limited available data.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.