

Summary
This article provides an overview of some of the latest results from clinical trials of drug-eluting stents (DES), issues surrounding stent thrombosis, as well as the mechanisms of DES failure.
- thrombotic disorders
- interventional techniques & devices
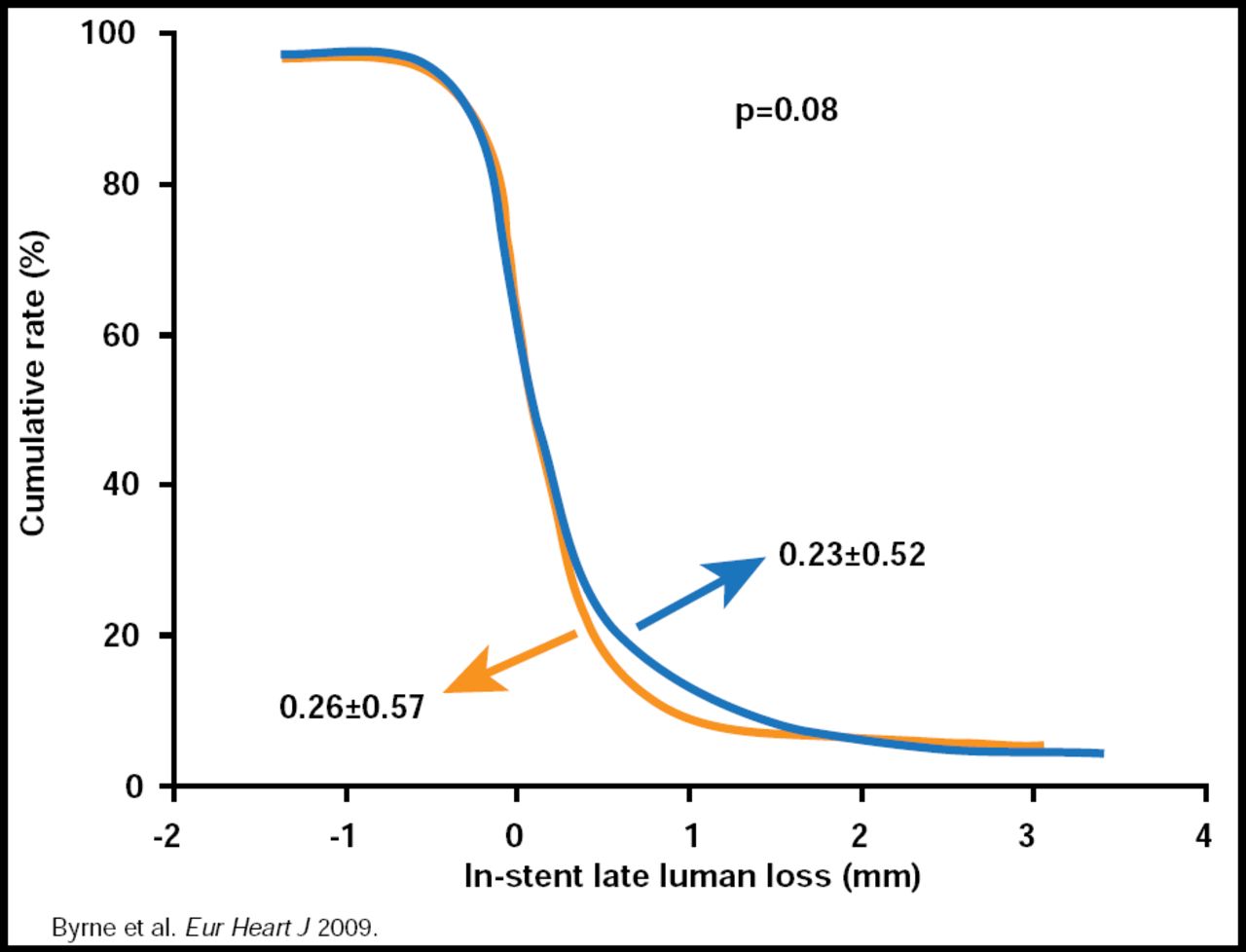
David J. Moliterno, MD, University of Kentucky, Lexington, KY, provided an overview of some of the latest results from clinical trials of drug-eluting stents (DES). The latest data from the Sirolimus-Eluting Stent [SES] Compared With Paclitaxel-Eluting Stent [PES] for Coronary Revascularization-Late (SIRTAX-LATE) study, presented by Lorenz Räber at TCT 2009, showed a narrowing of event curves between PES and SES by 5 years, primarily driven by target lesion revascularizations (TLRs), which were lower for SES up to Year 1 (HR, 0.54; 95% CI, 0.34 to 0.84; p<0.01) but similar between SES and PES at Year 5 (HR, 0.80; 95% CI, 0.59 to 1.52; p=0.16). One-year data from the ISAR-TEST-4 trial show similar results in terms of the outcomes of death, myocardial infarction (MI), TLR, or stent thrombosis between the everolimus-eluting stent (EES) and the SES but a trend toward fewer target vessel revascularizations (TVRs) and a somewhat lower rate of binary restenosis with EES (Figure 1) [Byrne RA et al. Eur Heart J 2009]. Unlike the initial one-year results that showed no difference, recently published 2-year data from the SPIRIT-III trial show significantly (p=0.04) fewer ischemic events with EES versus PES (10.7% vs 15.4%; HR, 0.68; 95% CI, 0.48 to 0.98) [Stone GW et al. Circulation 2009]. Similar results, in terms of fewer ischemic events with EES (vs PES) were also shown in both the SPIRIT-IV [Stone GW. TCT 2009] and COMPARE [Kehdi E et al. Lancet 2010] studies. Finally, 3-year results, presented at TCT 2009 and updated at ACC 2010, for the ENDEAVOR-IV study showed similar early events between zotarolimus-eluting stents (ZES) and PES but fewer later events with ZES. In closing, Dr. Moliterno noted that in addition to increased safety and efficacy, reduced cost has been an important advance in stent technology. Further, the advances have allowed clinicians to take on increasingly difficult cases.

ISAR-TEST 4.
DES are a major advance in the area of interventional cardiology, and most of the time, they work well; however, on occasion they do fail. Debabrata Mukherjee, MD, University of Kentucky, Lexington, KY, discussed the mechanisms of DES failure.
DES failure manifests as restenosis or stent thrombosis. Predictors of DES restenosis include female gender, prior coronary bypass surgery, minimal lumen diameter, lesion length >30 to 40 mm, and vessel and target lesion size [Lee CW et al. Am J Cardiol 2006; Kastrati A et al Circulation 2006; Berenguer A et al. Am Heart J 2005]. Potential mechanisms of restenosis include nonuniform drug delivery (eg, stent underexpansion, incomplete apposition, strut fracture, polymer disruption) and drug resistance or drug failure [Cowley MJ. J Interven Cardiol 2006]. Repeat PCI with another DES is currently the accepted treatment for DES restenosis.
Stent thrombosis likely also results from a combination of factors, including procedure- and patient-related factors and lesion characteristics. Predictors of stent thrombosis include stent malapposition and/or underexpansion, the number of implanted stents, stent length, persistent coronary blood flow, dissections, and premature cessation of antiplatelet therapy. In addition, some drugs that are loaded onto the stent may exert prothrombotic effects [Lüscher TF et al. Circulation 2007] and thus may increase the risk for stent thrombosis beyond that seen with BMS.
Preliminary data suggest that second-generation DES are safe and effective. Compared with BMS, they are associated with a similar long-term incidence of death and MI but provide a clinically important decrease in the rate of restenosis among high-risk patients.
The mechanisms of stent restenosis fall into three categories: biological (drug resistance, hypersensitivity), mechanical (stent fractures, polymer peeling, nonuniform stent strut distribution of drug deposition), and technical (incomplete stent expansion, gaps [uncovered lesion sections], and barotraumas to unstented segments). A tentative correlation has been established between these mechanisms and the site of DES restenosis [Costa MA et al. Circulation 2005] and between the pattern of restenosis and prognosis [Cosgrave J et al. J Am Clin Cardiol 2006]. Currently, results from only one randomized controlled trial in the treatment of DES restenosis have been presented [ISAR-DESIRE 2. Byrne R. TCT 2009]. Other trials that are currently enrolling include GISE-CROSS and CRISTAL.
“Understanding the mechanism of restenosis at time of treatment may impact the way you treat,” said George D. Dangas, MD, Columbia University, New York, NY. The treatment of DES restenosis should be based on appreciation of underlying mechanisms and can vary from simple balloon angioplasty to DES, when appropriate, to CABG (coronary artery bypass graft) in the most extreme cases (Table 1).
Current Therapeutic Options According to Potential Mechanisms of DES Restenosis.
Donald E. Cutlip, MD, Harvard Medical School, Boston, MA, closed this session with a discussion of some of the issues concerning stent thrombosis.
Data from randomized clinical trials indicate that the event rate for early (postprocedure to 30 days) and late (31 days to 1 year) stent thrombosis for both BMS and DES is between 0.5% and 1%, with the highest number being early stent thrombosis (Figure 2). The rate in clinical practice, which includes more complex or “off-label” cases, is just slightly higher, at between 1% and 1.5%, but still with the highest density of events within the first 30 days (Figure 2). Very late (>1 year) stent thrombosis in DES is infrequent (0.2% to 0.6% per year), with the newer stents appearing to have a slightly lower rate. “It's interesting to note that very late stent thrombosis occurs with BMS at just about the same rate as DES,” said Dr. Cutlip, “a fact that appears to have been missed in the early BMS clinical trials.”

Early and Late ST: RCTs and “Real World.”
Reproduced with permission from D. Cutlip, MD.
Stent thrombosis is predicted mostly by lesion and technical factors for up to about 1 year, with delayed healing the major factor thereafter. The risk factors are the same for both BMS and DES in the early and late periods, and although the risk factors for very late stent thrombosis are more biological, lesion factors still account for some instances. Several trials have indicated that there are differences in the occurrence of very late stent thrombosis among DES [Stone G; Smits P; Leon M. TCT 2009].
Patients who fail to have adequate response to clopidogrel after the loading dose have a 3-fold higher risk of stent thrombosis [Buonamici P et al. J Am Col Cardiol 2007], possibly due to the effect of the polymorphisms of the cytochrome P450 C219 allele on platelet activity [Mega JL et al. N Engl J Med 2009]. Although the optimal duration for dual antiplatelet therapy remains uncertain, discontinuation of dual antiplatelet therapy, particularly within the first 30 days and at least out to 6 months is a highly significant risk factor for thrombosis, with odds ratios approaching 50.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.