

Summary
According to long-term follow-up results from the Drug Elution and Distal Protection During Percutaneous Coronary Intervention in ST-Elevation Myocardial Infarction [DEDICATION; NCT00192868] trial, drug-eluting stents (DES) reduced the rate of major adverse cardiac events and were not associated with an increased rate of myocardial infarction or stent thrombosis compared with bare-metal stents. However, an increased incidence of cardiac death was observed in the DES group.
- interventional techniques & devices
- myocardial infarction clinical trials
According to long-term follow-up results from the Drug Elution and Distal Protection During Percutaneous Coronary Intervention in ST-Elevation Myocardial Infarction (DEDICATION; NCT00192868) trial, drug-eluting stents (DES) reduced the rate of major adverse cardiac events (MACEs) and were not associated with an increased rate of myocardial infarction (MI) or stent thrombosis compared with bare-metal stents (BMS). However, an increased incidence of cardiac death was observed in the DES group. Three-year data from the DEDICATION study was presented by Peter Clemmensen, MD, PhD, Copenhagen University Hospital, Copenhagen, Denmark.
Thus far, DES have demonstrated favorable results with regard to safety and efficacy compared with BMS in patients with coronary artery disease, particularly among those with stable conditions. However, there is limited long-term data available regarding DES use in patients with ST-elevation myocardial infarction (STEMI) who have undergone percutaneous coronary intervention (PCI). Early results from DEDICATION favored DES, but higher mortality rates were associated with DES at 8 months (overall mortality 5.1% for DES vs 2.6% for BMS at 8 months; p=0.14). Therefore, long-term evaluation was warranted in order to confirm the impact of DES on mortality and MACE rates over time.
The 3-year follow-up included 573 patients from the DEDICATION trial who presented with signs and symptoms of a first-time large STEMI, chest pain ≤12 hours duration, and ST-elevation >4 mm in contiguous leads and had high-grade stenosis/occlusion of a native coronary artery that could be crossed with a guidewire. Patients with a history of MI, left main stem stenosis, recent gastrointestinal bleeding (≤1 month), comorbidities with expected survival of <1 year, and linguistic difficulties that required the use of an interpreter were excluded from study participation. Patients were well matched at baseline, and ∼65% of patients in both groups had one vessel disease and Thrombolysis in Myocardial Infarction (TIMI) flow grade 0 to 1 at baseline.
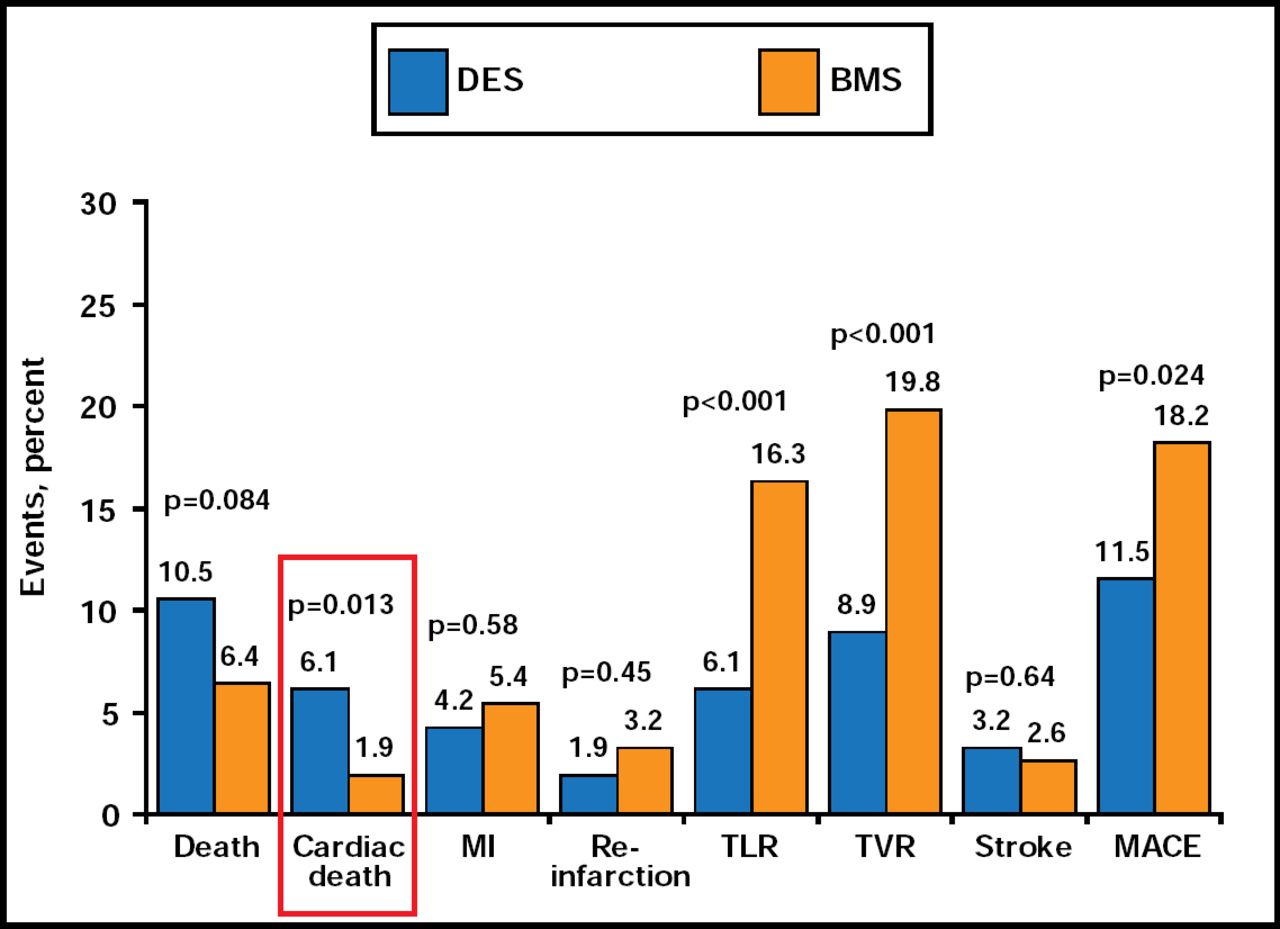
The endpoints were MACEs (defined as a composite of cardiac death, reinfarction, and total lesion revascularization), cardiac death, total mortality, MI, total lesion revascularization (TLR), total vessel revascularization (TVR), and stroke at 3 years. Overall, MACEs were less frequent in the DES group (11.5%) than in the BMS group (18.2%) at 3 years (p=0.024). However, the rate of cardiac death (6.1% vs 1.9% for BMS) and all-cause death (10.5% vs 6.4% for BMS) was higher in the DES group. The rates of TLR and TVR were significantly lower for DES compared with BMS (p<0.001 for both). There was no significant difference in the rates of MI or reinfarction between the two groups at 3 years (Figure 1).
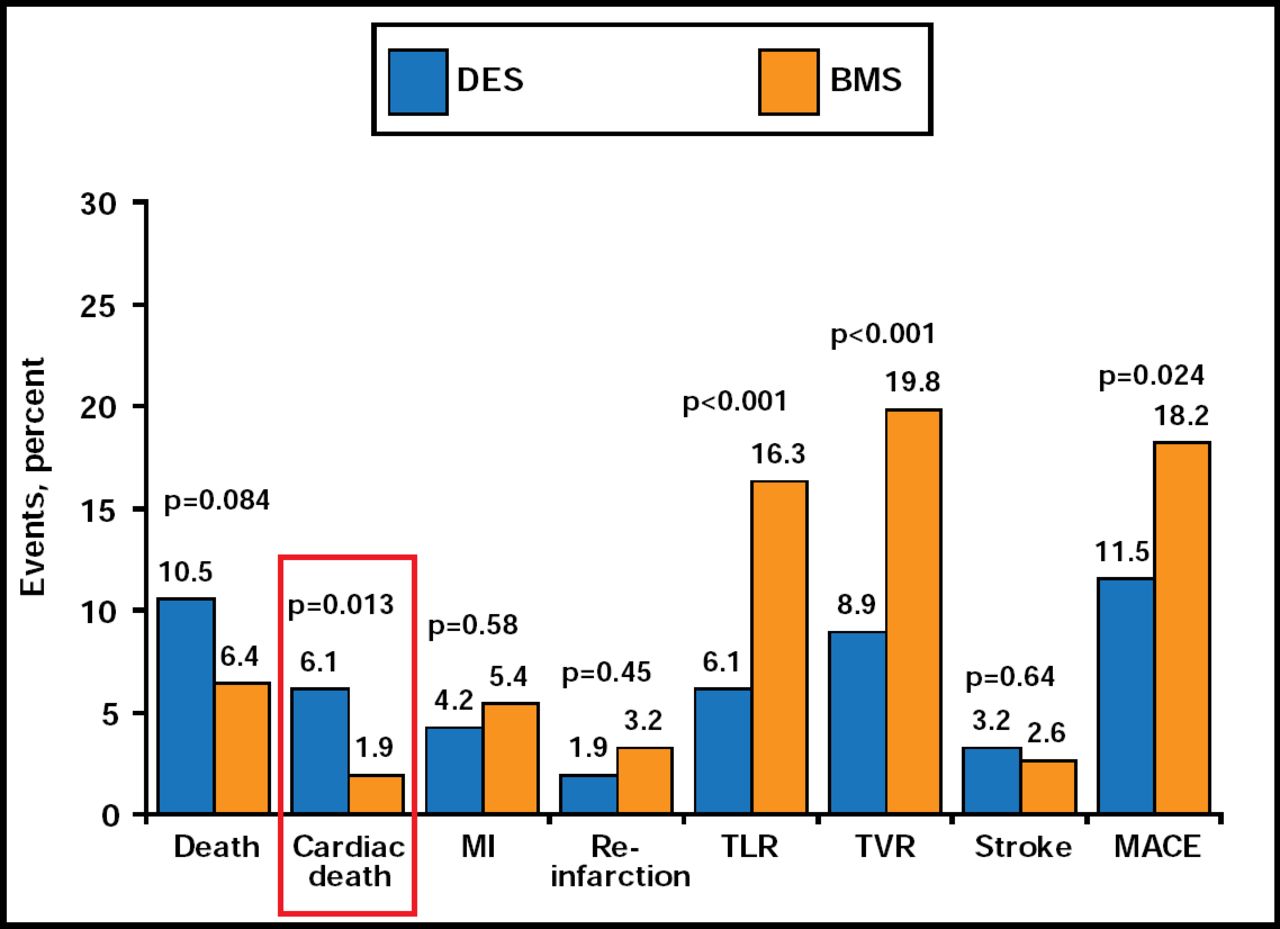
MACEs During 3 Years.
Reproduced with permission from P. Clemmensen, MD, PhD.
It is important to note that the incidence of stroke was similar between the two groups at 3 years. Though the general theory has been that DES lead to more stent thromboses, this was not the case in the DEDICATION trial, Prof. Clemmensen concluded. DES effectively reduced the rate of MACEs and the need for repeat revascularization in STEMI patients without associated increases in the incidence of MI or stent thrombosis. The increased risk of cardiac death that was associated with DES merits further investigation and should be considered before choosing a treatment strategy.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.