

Summary
Rheolytic thrombectomy plus stenting is associated with better 6-month outcomes and improved myocardial reperfusion compared with direct stenting alone in patients with ST-elevation myocardial infarction. While procedure time was higher in the thrombectomy group (60 minutes) than in the direct stenting group (46 minutes; p<0.001), this did not appear to impact the rate of procedural complications, such as the need for pacing to vessel perforation. This article discusses results from the Comparison of Angiojet Rheolytic Thrombectomy Before Direct Infarct Artery Stenting to Direct Stenting Alone in Patients with Acute Myocardial Infarction [JETSTENT; NCT00275990[Trial].
- myocardial infarction
- thrombotic disorders
- interventional techniques & devices clinical trials
Rheolytic thrombectomy plus stenting is associated with better 6-month outcomes and improved myocardial reperfusion compared with direct stenting alone in patients with ST-elevation myocardial infarction (STEMI). While procedure time was higher in the thrombectomy group (60 minutes) than in the direct stenting group (46 minutes; p<0.001), this did not appear to impact the rate of procedural complications, such as the need for pacing to vessel perforation. David Antoniucci, MD, Careggi Hospital, Florence, Italy, discussed results from the Comparison of Angiojet Rheolytic Thrombectomy Before Direct Infarct Artery Stenting to Direct Stenting Alone in Patients with Acute Myocardial Infarction (JETSTENT; NCT00275990) Trial.
The JETSTENT study included 500 patients with STEMI within 12 hours of symptom onset, at least moderate thrombus burden, and infarct artery vessel diameter ≥2.5 mm. Patients were randomized to either rheolytic thrombectomy (RT) plus stenting (n=256) or direct stenting (DS) alone (n=245). The use of a temporary pacemaker and balloon predilation was strongly discouraged. Patients with recent stroke (≤30 days), recent surgery (≤6 weeks), a prestented infarct-related artery, or lysis were excluded from participation in the study. However, cardiogenic shock was not grounds for exclusion and accounted for 2.7% of patients in the RT group and 5.3% of patients in the DS group. The mean follow-up was 6 months, and the mean age was 63 years. Patients were well matched at baseline.
The primary surrogate endpoints were early ST-segment resolution, defined as ≥50% reduction in ST-segment elevation at 30 minutes, and final infarct size at one month, determined by scintigraphy. Clinical endpoints were major adverse cardiac events (MACEs) at 1, 6, and 12 months and death or readmission for congestive heart failure at 12 months. The secondary surrogate endpoints included Thrombolysis in Myocardial Infarction (TIMI) flow, corrected TIMI frame count, and TIMI blush grade.
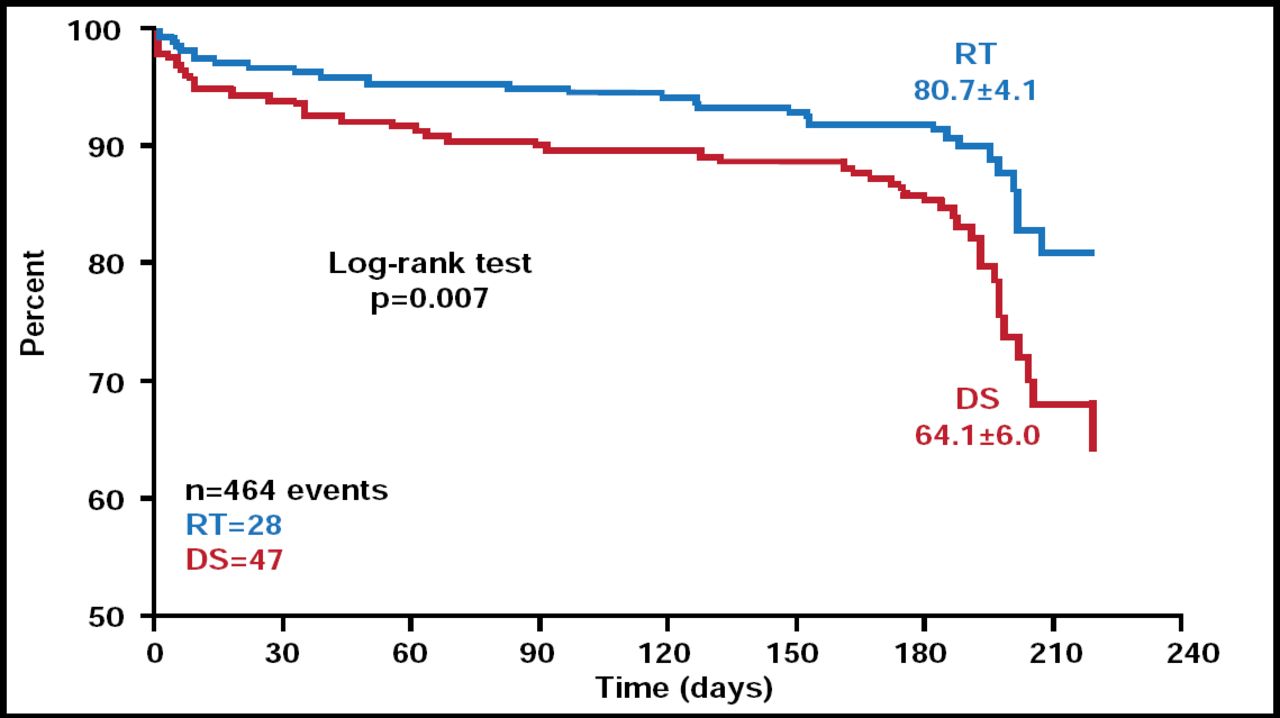
There was no significant difference in final infarct size between RT and DS (p=0.40). However, ST-segment resolution at 30 minutes was significantly improved in patients who underwent RT compared with DS (p=0.04). However, anterior acute MI appeared to be a predictor of ST-segment resolution (p<0.001). At one month, there was a 2-fold increase in MACEs in patients who received DS compared with RT (6.9% vs 3.1% for RT; p=0.05). DS was also associated with higher rates of death, MI, total vessel revascularization, and stroke compared with RT at one month. This trend continued at 6 months, with the exception of stroke incidence, which was identical in both groups (0.4% for both). TIMI major bleeding occurred in 3.9% of RT patients versus 1.6% of DS patients (p=0.12). However, this difference did not reach statistical significance. Total MACE rate at 6 months was 20.7% for the DS group versus 12.0% for the RT group (p=0.01). Randomization to RT, age, and bleeding appeared to be predictors of MACEs at 6 months (Figure 1).

6-Month MACE Kaplan-Meier Estimate.
Reproduced with permission from D. Antoniucci, MD.
The JETSTENT trial demonstrated benefit for RT use in patients with STEMI. This strategy is associated with higher rates of early ST-segment resolution and improved clinical outcomes at 6 months. These improvements occurred without any apparent increase in stroke or major bleeding. Further evaluation is required to confirm the long-term safety and efficacy of this strategy.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.