

Summary
Increased intensity of rehabilitation is associated with better motor recovery in stroke patients [Kwakkel G et al. Stroke 1997]. However, the effectiveness of interactive virtual reality gaming (such as that found with the Nintendo Wii system) for stroke rehabilitation remains unclear. This article presents results from the randomized, single-blinded, Effectiveness of Virtual Reality Exercises in Stroke Rehabilitation [EVREST; NCT00692523] study, which investigated this issue.
- cerebrovascular disease
- nursing
- neurology clinical trials
Increased intensity of rehabilitation is associated with better motor recovery in stroke patients [Kwakkel G et al. Stroke 1997]. However, the effectiveness of interactive virtual reality gaming (such as that found with the Nintendo Wii system) for stroke rehabilitation remains unclear. Gustavo Saposnik, MD, St. Michael's Hospital, Toronto, Ontario, Canada, presented results from the randomized, single-blinded, Effectiveness of Virtual Reality Exercises in Stroke Rehabilitation (EVREST; NCT00692523) study, which investigated this issue.
Twenty-two patients (mean age=61 years) who received standard rehabilitation within 2 months after a mild to moderate stroke (defined as arm deficit of ≥4 on the Chedocke-McMaster scale) were randomized to receive either virtual reality therapy using the Wii system (VRWii; n=11) or recreational therapy (RT; n=11), such as playing cards or Jenga, for eight 60-minute sessions over a 2-week period. Comorbidities included hypertension, dyslipidemia, diabetes mellitus, and atrial fibrillation. Functional status at the time of randomization for the VRWii group included a mean Canadian Neurological Scale of 8.5 (vs 9.7 in the RT group), median Chedocke-McMaster score of 4.0 (vs 4.5 for RT), and a median Barthel Index of 65 (for both groups). A modified Rankin Scale (mRS) of 3 to 4 was noted in 81% of VRWii patients and 63% of RT patients at baseline. The mean time from stroke onset to randomization was 24 days, and baseline characteristics were similar in both groups. Patients in both groups were instructed to use their affected arm predominantly. The primary outcomes were the total time receiving the intervention (assessing feasibility) and the proportion of patients who were experiencing intervention-related adverse events during the study period (assessing safety). The secondary outcome was efficacy, as determined by Wolf Motor Function Test (WMFT), Box and Block Test (BBT), and the Stroke Impact Scale (SIS), performed at a follow-up visit 4 weeks postintervention.
No serious adverse events were observed. Dizziness/ nausea was noted in one patient in the RT group but none in the VRWii group. Fatigue, determined as Borg scale >13, was observed in 3 patients in the VRWii group versus 2 for RT. Four patients in the RT group reported any symptom during any session versus 6 in the VRWii group.
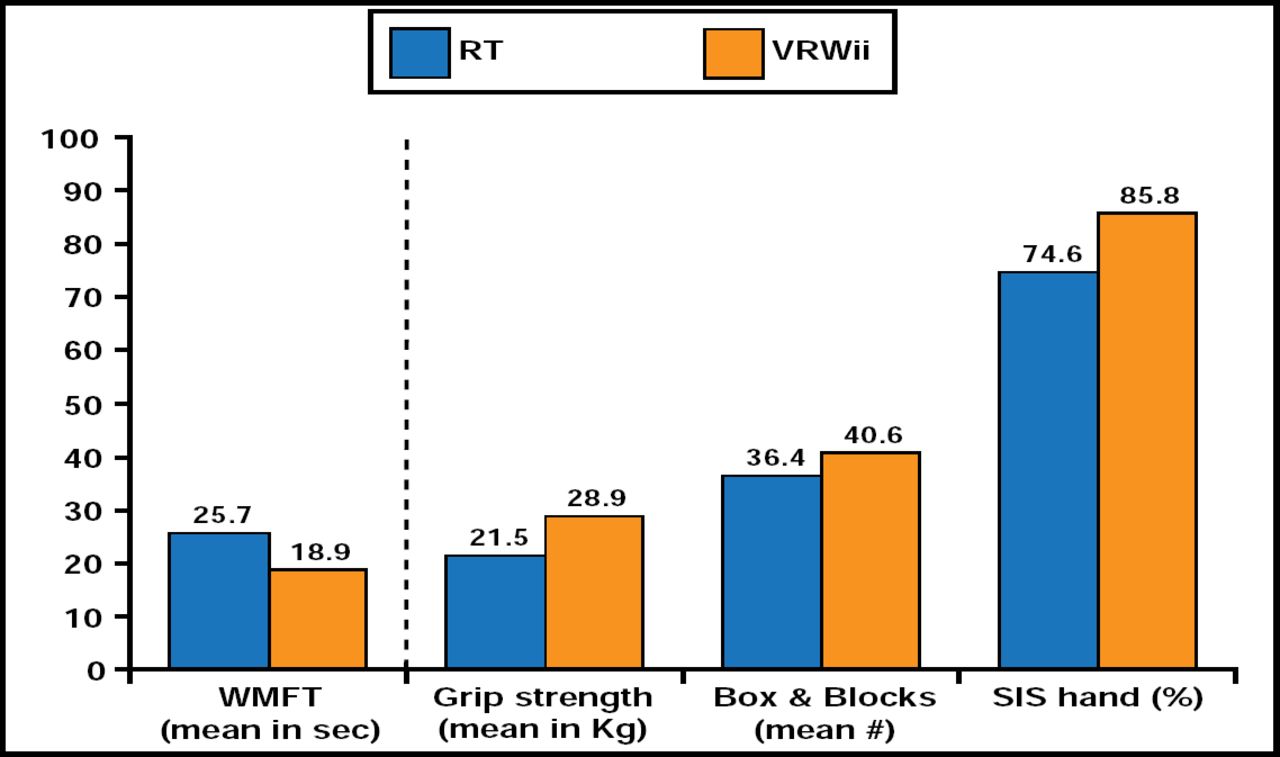
Eighty percent of patients in the RT group completed all 8 sessions versus 90% of patients in the VRWii group. The mean total session time was 364 minutes and 388 minutes for VRWii and RT, respectively. The mean individual session time was 46.5 minutes and 56.2 minutes for VRWii and RT, respectively. Patients in the VRWii group did significantly better on the WMFT postintervention after adjustment for age, baseline functional status, and stroke severity compared with the RT group. The VRWii group also demonstrated improvement in grip strength, BBT, and SIS at 4 weeks (Figure 1).
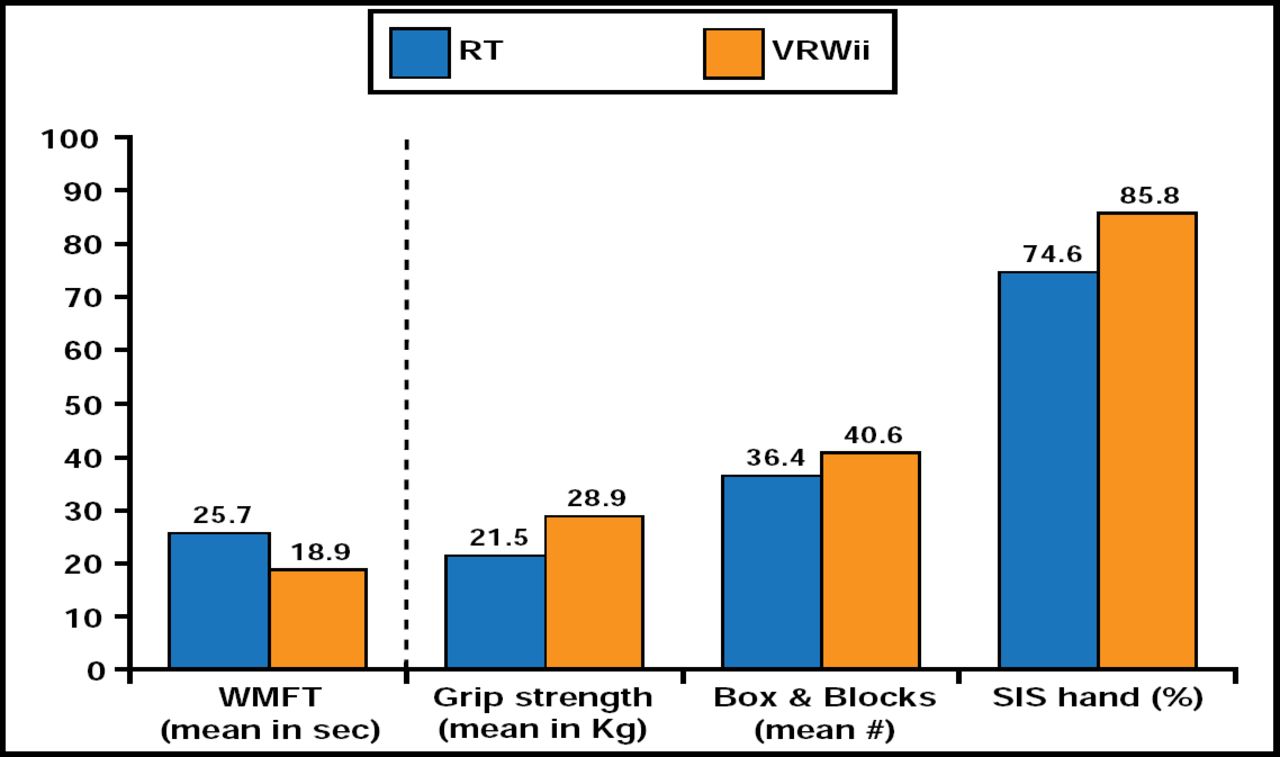
Unadjusted Secondary Outcomes (Efficacy).
Reproduced with permission from G. Saposnik, MD.
VRWii may be a useful strategy for home rehabilitation that is focused on promoting motor function after stroke. This innovative interactive approach appears to be safe, feasible, and potentially effective in enhancing motor function after an acute stroke, concluded Dr. Saposnik.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.