

Summary
This article discusses new data from a substudy of the REGARDS Study that suggested that unrecognized myocardial infarction and recognized myocardial infarction confer a similar risk of stroke and that the former, in particular, is a risk factor for future stroke in those with prevalent stroke.
- Neurology
- Prevention & Screening
- Myocardial Infarction
- Cerebrovascular Disease
Previous publications from the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study examined traditional risk factors for stroke and coronary heart disease among African-Americans and people living in the southeastern United States [Cushman M et al. Ann Neurol 2008]. Aaron Anderson, MD, Emory University, Atlanta, Georgia, discussed new data from a substudy of REGARDS that suggested that unrecognized myocardial infarction (UMI) and recognized MI confer a similar risk of stroke and that UMI, in particular, is a risk factor for future stroke in those with prevalent stroke.
Participants in the REGARDS study included 30,239 community-dwelling black and white men and women ≥45 years (50% white, 50% black) who were recruited by phone. In-home examinations, blood collections, ECGs, and anthropometric measurements were performed. Follow-up phone calls were made every 6 months to ascertain a stroke event (defined as a self-reported stroke, transient ischemic attack [TIA], or stroke symptom) or death.
Participants in this substudy were classified as having UMI (n=923), recognized MI (n=1534), or no MI (n=18,055). UMI participants were defined as those individuals who had ECG evidence of MI per Minnesota Code criteria who answered either “no” or “don't know” to the question, “Has a doctor or other health professional ever told you that you had a myocardial infarction or heart attack?” Subjects with self-reported MI were classified as having recognized MI, and those without a self-report of MI or ECG evidence of MI were considered as having no MI. There was a higher percentage of black participants in the UMI group (41.7%) compared with the no-MI (40.9%) and recognized-MI groups (37.5; p=0.028). The recognized-MI group had the highest percentage of men and participants with the traditional risk factors for stroke, such as diabetes, hypertension, and being a current smoker. Level of education and income were highest in the no-MI group and lowest in the recognized-MI group.
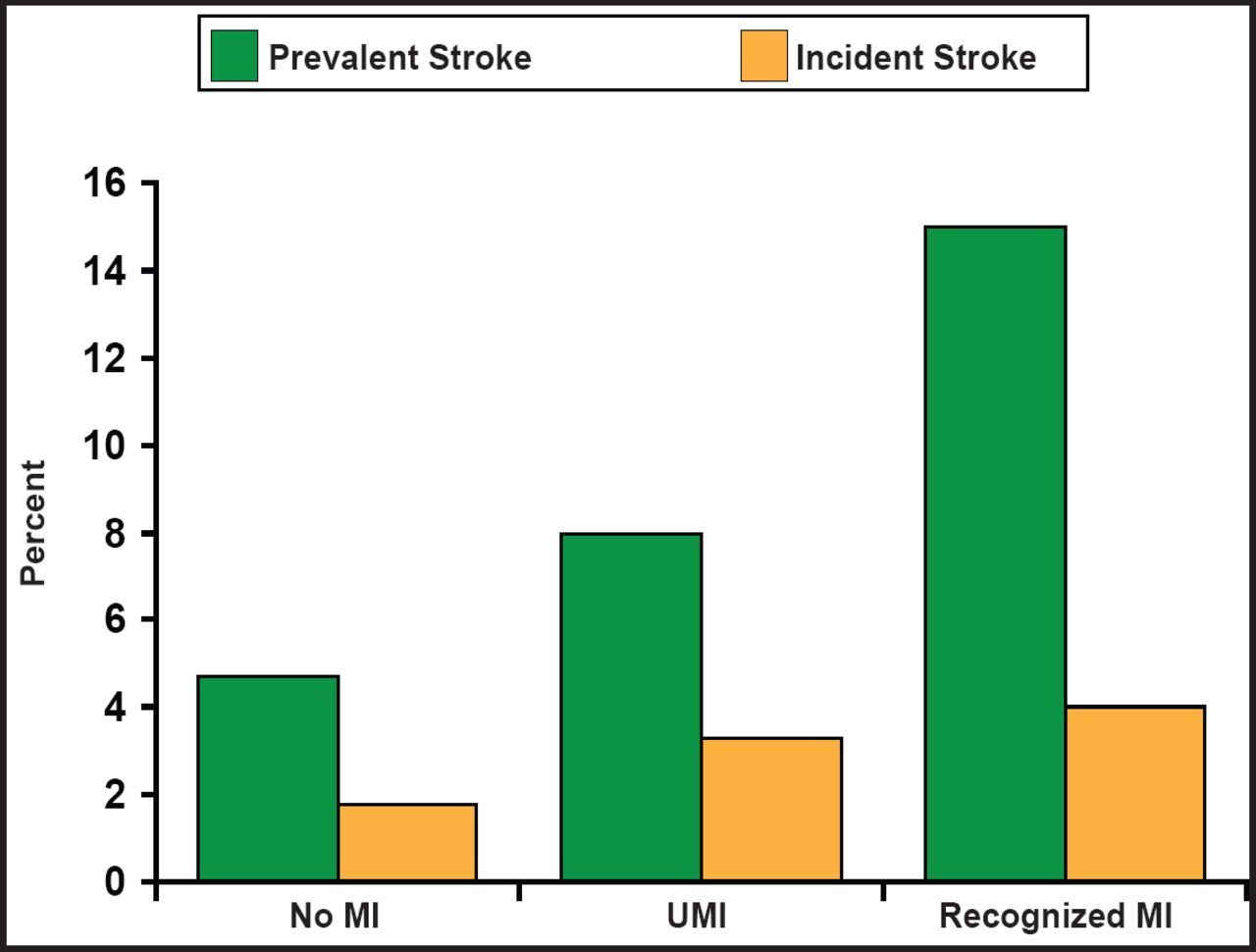
The rate of prevalent stroke was higher in both the recognized-MI and the UMI groups compared with the no-MI group. The rate of incident stroke was similar between the UMI and the recognized-MI groups, but both were significantly higher than in the no-MI group (Figure 1).

Proportion of Participants with Prevalent and Incident Stroke
Reproduced with permission from A. Anderson, MD.
Time-to-event analyses were performed to determine if prevalent stroke modified the risk between UMI and MI. Those individuals with prevalent stroke had double the risk (RR, 2.69; 1.48, to 4.77) of incident stroke with a UMI. However, participants with a recognized MI and no history of stroke or TIA also had twice the risk (RR, 2.21; 1.56 to 3.12) of stroke. After adjusting these findings for age, race, gender, income, education, age-race interaction, diabetes, hypertension, and smoking, the differences in risk remained. The investigators suggested that the difference may be explained by the potential for subjects with recognized MI to have a cardioembolic stroke compared with subjects with a prevalent stroke and UMI whose stroke may have been the result of underlying atherosclerosis. The differences might also be explained by medication management or the collaborative effort among specialists to treat patients with recognized MI and prevalent stroke that is not provided to UMI participants.
This study may be limited by the possibility that participants may have been previously diagnosed by a physician or health care professional but had poor recollection when questioned or had suffered cognitive decline in the interim.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.