

Summary
Among patients with atrial fibrillation (AF) treated with anticoagulants, differences in baseline characteristics only partially account for the differences in outcome by AF subtype. This article presents results of a secondary data analysis from the Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation—Thrombolysis in Myocardial Infarction 48 trial [ENGAGE AF-TIMI 48; NCT00781391].
- Cardiology Clinical Trials
- Arrhythmias
- Cerebrovascular Disease
- Cardiology Clinical Trials
- Arrhythmias
- Cerebrovascular Disease
- Cardiology & Cardiovascular Medicine
Among patients with atrial fibrillation (AF) treated with anticoagulants, differences in baseline characteristics only partially account for the differences in outcome by AF subtype. Robert P. Giugliano, MD, SM, Brigham and Women's Hospital, Boston, Massachusetts, USA, presented results of a secondary data analysis from the Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48 trial [ENGAGE AF-TIMI 48; NCT00781391]. These results showed that therapies that reduce bleeding while maintaining efficacy in the prevention of stroke (as compared with warfarin) may be especially beneficial in patients with paroxysmal AF.
Edoxaban is a direct, oral, once-daily Factor Xa inhibitor. In the ENGAGE AF-TIMI 48 trial, both high and low doses of edoxaban were at least as effective as warfarin in preventing stroke and systemic embolic events (SEE) in patients with AF at moderate to high risk of stroke and caused less bleeding [Giugliano RP et al. N Engl J Med 2013].
The objective of the secondary analysis was to compare the baseline characteristics by AF subtype at presentation and compare the efficacy and safety of edoxaban by subtype during the 2.8 years median follow-up using the primary efficacy and safety outcomes from the main trial (efficacy=stroke or SEE; safety=ISTH major bleeding). Additional key secondary trial end points were also considered. For the ENGAGE AF-TIMI 48 trial, 21,105 patients with documented AF of any duration during the prior 12 months and a CHADS2 score of greater than or equal to 2 were enrolled. For this secondary analysis, patients were categorized as having paroxysmal (n=5366 patients), persistent (n=4868), or permanent (n=10,865) AF based on the randomization ECG.
Patients with paroxysmal AF were more likely to be younger and female, to have a higher rate of diabetes, a lower CHADS2 score, to have a history of coronary artery disease or dyslipidemia, and to be receiving antiarrhythmic therapy. Patients with permanent AF were slightly older and more were likely to have a higher CHADS2 score and heart failure, as well as a higher incidence of prior stroke. They were also less likely to be vitamin K antagonist therapy-naïve.
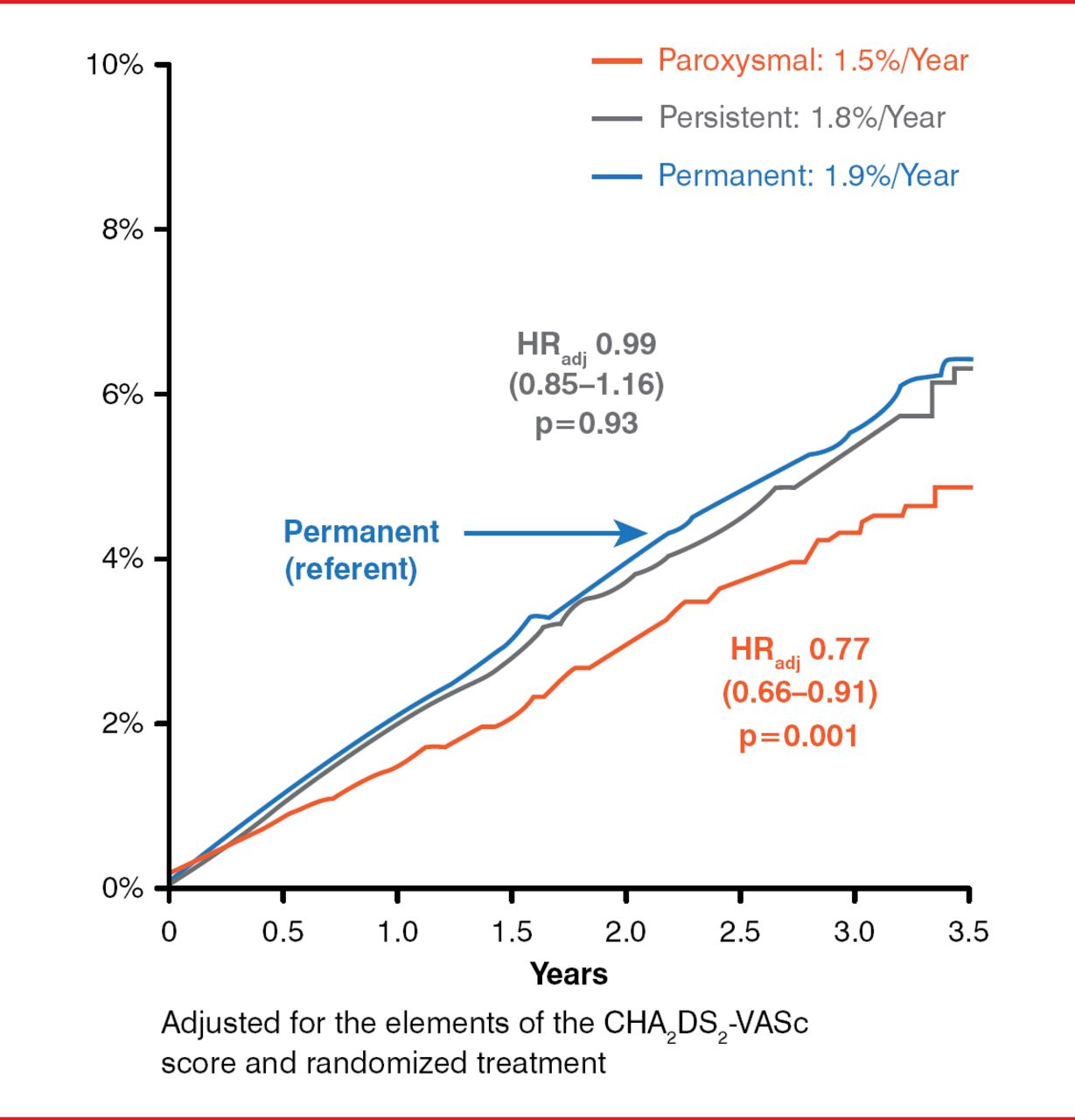
The rate of stroke or SEE adjusted for elements of the CHA2DS2-VASc score, the group with paroxysmal AF was 23% lower in patients with paroxysmal AF as compared to permanent AF (adjusted HR, 0.77; 95% CI, 0.66–0.91; p=0.001); there was no difference in the rate of stroke or SEE between the permanent and persistent groups (Figure 1). Regarding the primary safety outcome, the adjusted rates for major bleeding were similar across all three groups.

Primary Efficacy Outcome by AF Subtype
SEE=systemic embolic events.
Reproduced with permission from RP Giugliano, MD.
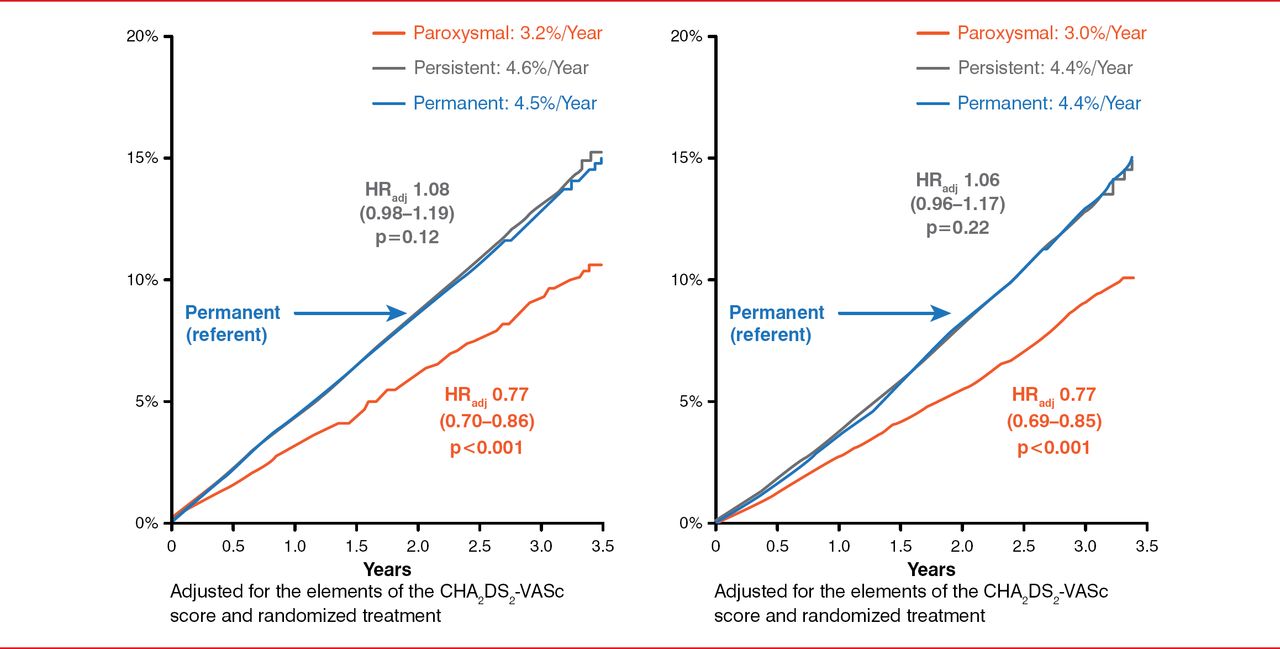
Compared with subjects with permanent AF, subjects in the paroxysmal group had a lower risk for the key combined secondary outcome of stroke plus SEE plus cardiovascular death after adjusting for the CHA2DS2-VASc score (adjusted HR, 0.77; 95% CI, 0.70–0.86; p<0.001). There was no difference between the permanent and persistent groups (Figure 2). The outcome was similar for mortality, with patients in the paroxysmal group having a 23% reduction in the adjusted HR for death and no difference between patients with permanent versus persistent AF (Figure 2).

Key Secondary Outcomes by AF Subtype
CV=cardiovascular; SEE=systemic embolic events.
Reproduced with permission from RP Giugliano, MD.
The risk for cardiovascular death was approximately 25% lower and the risk for the primary net outcome (stroke, SEE, major bleeding, or death) was approximately 13% lower in the paroxysmal group versus the permanent group after adjustment. There was no difference in the outcomes for intracranial hemorrhage. The results described for subjects with persistent AF were not different from those described for patients with permanent AF (Table 1).
Other Outcomes by AF Subtype
Efficacy outcomes (stroke or SEE; combined stroke, SEE and cardiovascular death; all-cause mortality; or cardiovascular death) were similar between patients treated with edoxaban and those treated with warfarin regardless of the edoxaban dose (high versus low dose) or AF subtype. With respect to safety, there was a reduction in the proportion of patients who had major bleeding, those who had a combination of stroke, SEE, major bleeding and death, and, in particular, those patients who had intracranial hemorrhage with both doses of edoxaban for all AF subtypes.
In conclusion, patients with paroxsymal AF were at a lower risk for stroke or SEE but had a similar risk of bleeding as patients with more sustained AF. Compared with patients with well-managed warfarin dosages (time in therapeutic range of 68.4%), edoxaban was associated with a reduced incidence of stroke or SEE, cardiovascular death, and bleeding, as well as more favorable net outcomes across all AF subtypes.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.