

Summary
This article discusses dietary prevention strategies, the role of hormones in cancer prevention, and the interception approach of cancer prevention.
- Gastrointestinal Cancers
- Breast Cancer
- Gastrointestinal Cancers
- Breast Cancer
- Oncology
No randomized controlled trials have evaluated the effect of diet in the prevention of cancer or during cancer treatment. Therefore, there is confusion among clinicians and the public about the role of diet in cancer prevention. Jeffrey A. Meyerhardt, MD, MPH, Dana-Farber Cancer Institute, Boston, Massachusetts, USA, discussed dietary prevention strategies.
A higher body mass index is associated with a greater risk of death from multiple types of cancer [Calle EE et al. N Engl J Med 2003]. In addition, consumption of red meat and processed meat is associated with an increased risk of cancer mortality, whereas the consumption of white meat appears to have a protective effect [Sinha R et al. Arch Intern Med 2009]. Furthermore, an expert report by the World Cancer Research Fund and the American Institute for Cancer Research indicated that red meat and processed meat increase the risk of colorectal cancer and that Cantonese-style salted fish increases the risk of nasopharyngeal cancer [WCRF/AICR 2007]. A meta-analysis showed that higher consumption of red and processed meat is associated with an increased relative risk of developing colorectal cancer [Chan DS et al. PLoS ONE 2011].
The benefit of fruit and vegetable intake is less clear. A pooled multivariate analysis did not suggest a significant benefit of fruit or vegetable consumption in the development of breast cancer [Jung S et al. J Natl Cancer Inst 2013]. Similarly, a meta-analysis did not yield a significant effect of fruit or vegetable consumption and the risk of developing pancreatic cancer in men or women [Koushik A et al. Am J Epidemiol 2012]. Another meta-analysis revealed mixed results for the association of fruit and vegetable intake and the risk of colon cancer, with a pooled relative risk of 0.91 (95% CI, 0.82 to 1.01) [Koushik A et al. J Natl Cancer Inst 2007].
Randomized clinical trials with supplemental β-carotene failed to show a benefit in the prevention of lung cancer. In fact, CARET and the ATBC trial revealed an increased incidence of lung cancer in patients who received β-carotene supplements compared with placebo [Omenn GS et al. N Engl J Med 1996; ATBC Cancer Prevention Study Group. N Engl J Med 1994]. A study of patients with colorectal cancer found that high-tertile (median, 31.0 ng/mL) serum vitamin D levels were associated with survival over 12 years (log rank p<0.04) [Ng K et al. Br J Cancer 2009].
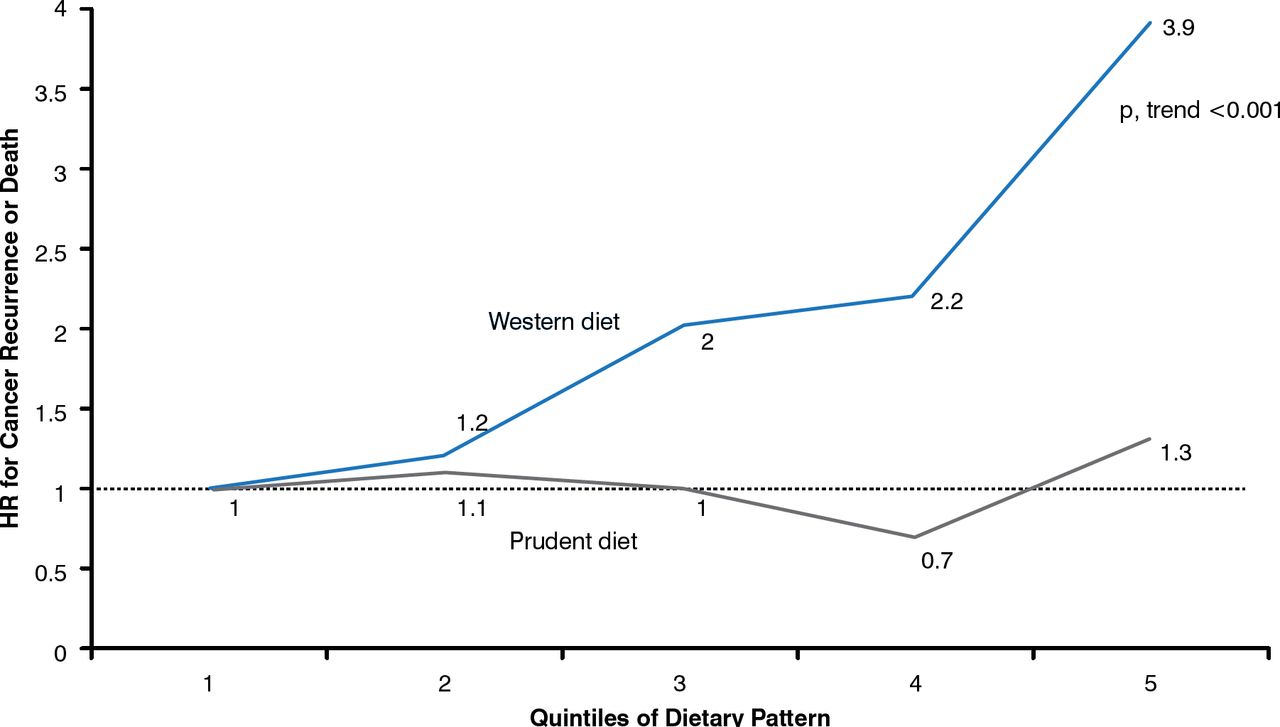
The effect of diet on cancer outcome or recurrence is also uncertain. Although multiple studies have indicated that a high-fat diet is associated with a poor prognosis in women with breast cancer, many studies have also showed no effect. However, women with breast cancer who participated in the WINS trial and decreased their fat to 8% of calories, resulting in a mean decrease in body weight of 2.7 kg, experienced a decrease in disease-free survival, which was particularly evident in patients with estrogen receptor– and progesterone receptor–negative disease [Chlebowski RT et al. J Natl Cancer Inst 2006]. A Western-style diet—including high total carbohydrates, high glycemic load, and high consumption of sugar-sweetened beverages—is associated with cancer recurrence or death (Figure 1) [Meyerhardt JA et al. J Natl Cancer Inst 2012].

Western Diet and Risk of Colon Cancer Recurrence or Death
Reproduced with permission from JA Meyerhardt, MD.
Victor G. Vogel, MD, MHS, Geisinger Health System, Danville, Pennsylvania, USA, presented on the role of hormones in cancer prevention. Preventative therapy with tamoxifen, a selective estrogen receptor modulator (SERM), has been shown to reduce the risk of invasive breast cancer in high-risk women. The SERM raloxifene also reduces the risk of invasive breast cancer in high-risk women, albeit to a lesser extent than tamoxifen. However, tamoxifen is associated with a greater rate of endometrial cancer and thrombotic events. A benefit-risk assessment of the 5-year projected risk for invasive breast cancer revealed that the benefits of tamoxifen outweigh the risk when the 5-year projected risk of invasive breast cancer reaches 4.5 in women aged 50 to 59 years [Freedman AN et al. J Clin Oncol 2011]. The benefits of raloxifene outweigh the risk when it reaches 2.0 in patients aged 50 to 59 years. The aromatase inhibitors (AIs) anastrozole and exemestane have also been shown to reduce the risk of invasive breast cancer.
Despite the risk reduction in invasive breast cancer with SERM or AI treatment in high-risk women, uptake has been low, likely as a result of lack of training in the benefit-risk counseling technique, lack of reimbursement, insufficient time, and concerns of side effects.
William Nassib William Jr, MD, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA, discussed the interception approach of cancer prevention. This approach attempts to use rational selection of effective agents to target early molecular drivers of cancer. In addition, Dr. William advocated reverse migration, in which drugs and strategies used to treat advanced cancers can be migrated to the premalignancy setting, thus preventing invasive tumors [Gold KA. Cancer Prev Res (Phila) 2011].
A challenge of chemoprevention is determining the population that is at highest risk for cancer and would theoretically benefit more from an intervention. One study indicated that loss of heterozygosity (LOH) at certain chromosomal sites is associated with an increased risk of developing cancer in patients with oral premalignant lesions [Mao L et al. Nat Med 1996], and these findings were corroborated in independent cohorts of patients with oral premalignant lesions, with or without a history of oral cancer [Rosin M et al. Clin Cancer Res 2000; Rosin M et al. Cancer Res 2002; Zhang et al. Cancer Prev Res (Phila) 2012]. As a result of these findings, the Erlotinib Prevention of Oral Cancer trial [EPOC; NCT00402779] was initiated, in which patients with oral premalignant lesions harboring high-risk LOH profiles, with or without oral cancer history, were randomly assigned to receive erlotinib or placebo. Over 72 months of follow-up, erlotinib treatment did not improve oral cancer–free survival in patients with LOH compared with placebo; nevertheless, a first-month rash was associated with survival among patients who received erlotinib [William WN et al. J Clin Oncol 2014].
Although some aspects of cancer prevention have been associated with reduced incidence, such as SERM or AI use for the prevention of invasive breast cancer, uptake of chemoprevention is low. In addition, more data are needed to determine role of diet and supplements in the prevention of cancer.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.