

Summary
EUROASPIRE III and IV findings were compared to gauge changes in lifestyle/risk factor management and therapeutic control in high-risk cardiovascular disease patients. Little progress was apparent in reducing smoking and prevalence of overweight/obese individuals, increasing physical activity, and improving therapeutic control of risk factors. Preventive cardiology programs are still needed.
- cardiovascular disease
- EUROASPIRE
- interventions
- obesity
- therapuetic control
Lifestyle modification and aggressive risk factor control continue to be a priority for those at high risk of developing cardiovascular diseases (CVDs), according to the EUROASPIRE III and IV surveys conducted in 2006-2007 and 2013-2015, respectively. The continuing bleak outlook was summarized by Kormelia Kotseva, MD, Imperial College London, London, UK.
The EUROASPIRE surveys concerned with CVD prevention—which began in 1995 under the auspices of the European Society of Cardiology, Euro Heart Survey, and subsequently the EURObservational Research Programme—have been designed to identify risk factors in coronary patients and individuals at high risk for CVD, to clarify patient management through lifestyle modifications and drugs, and to assess how effectively current knowledge is being used in general practice. Here, the EUROASPIRE III and IV findings were compared to better gauge the changes that had occurred in lifestyle/risk factor management and the use of cardioprotective drugs in people at high risk of developing CVD.
EUROASPIRE III and IV involved a total of 3827 patients (Table 1).
Study Population of EUROASPIRE III and IV
Consecutive men and women < 80 years old from Bulgaria, Croatia, Poland, Romania, and the UK with no history of coronary or other atherosclerotic disease were included. Medications prescribed ≥ 6 months and ≤ 3 years prior to survey participation included drugs intended to lower blood pressure, lipid, and/or glucose. Height, weight, waist circumference, blood pressure, breath carbon monoxide, and analyses of fasting venous blood for parameters including serum total cholesterol, high-density lipoprotein cholesterol, calculated low-density lipoprotein cholesterol, triglycerides, glucose, and glycated hemoglobin were done with the same protocols and instruments and in the same geographic regions, permitting direct comparison of survey data.
The overall prevalence of smoking remained constant at 17%. However, there were marked variations, including a 17–percentage point increase in Bulgaria (5% to 22%), decreases of about 9 points in both Poland (31% to 22%) and Romania (18% to 9%), and no change in the UK. Overall, the prevalence of current smokers with no intention to quit rose by 11 percentage points, from 23% in EUROASPIRE III to 34% in EUROASPIRE IV (P = .004).
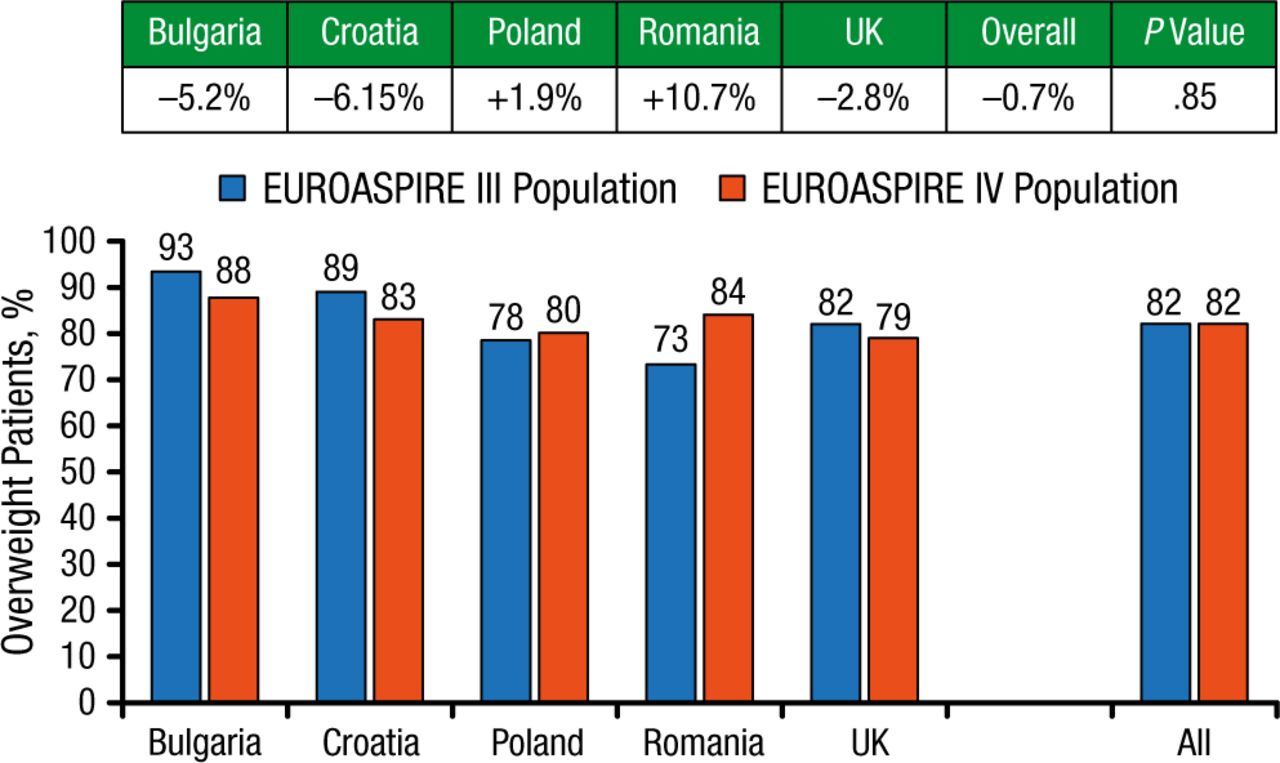
The prevalence of individuals defined as being overweight (body mass index ≥ 25 kg/m2) was high in both surveys (82%; Figure 1).
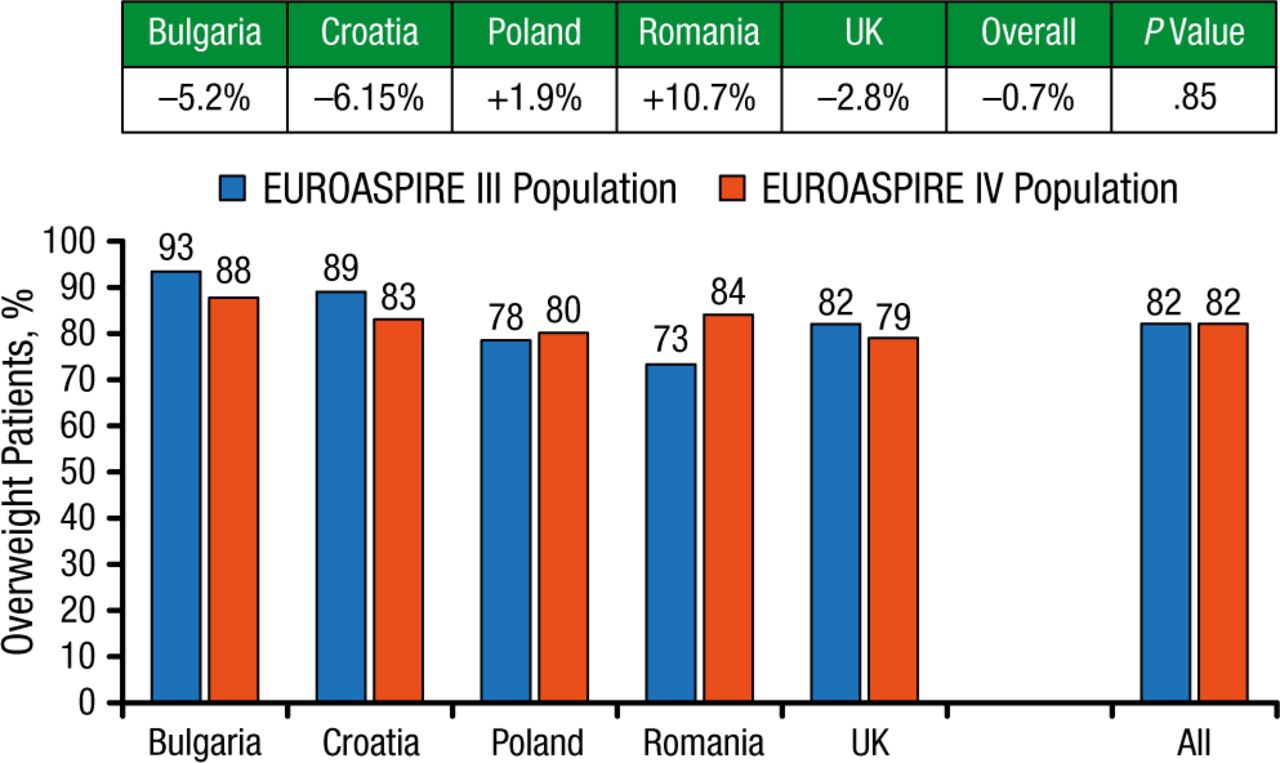
Prevalence of Overweight
Reproduced with permission from K Kotseva, MD.
Overall, central obesity, defined as waist circumference ≥ 88 cm in women and ≥ 102 cm in men, increased by 6 percentage points (P = .052). Obese patients who had been told that they were overweight and who were counseled by a health care professional concerning an unhealthy diet composed 56% and 73% of the EUROASPIRE III survey and 54% and 71% of the EUROASPIRE IV survey, respectively. Overall, the prevalence of obese patients trying to lose weight and those contemplating weight loss at the time of survey rose by only 4 and 1 percentage point(s), respectively, from 2007 to 2015 (P = .34 and .86, respectively). Variations among countries were evident.
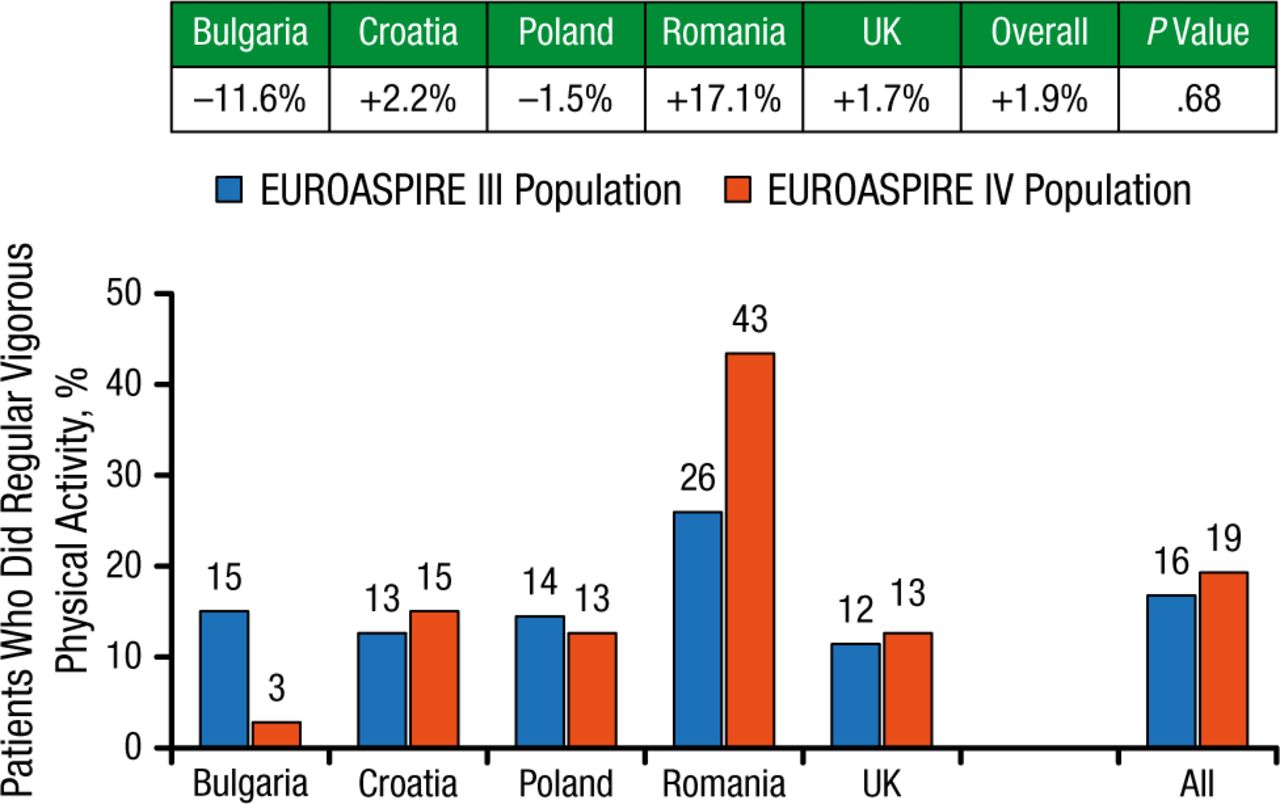
Exercise was generally not a widely adopted practice (Figure 2).
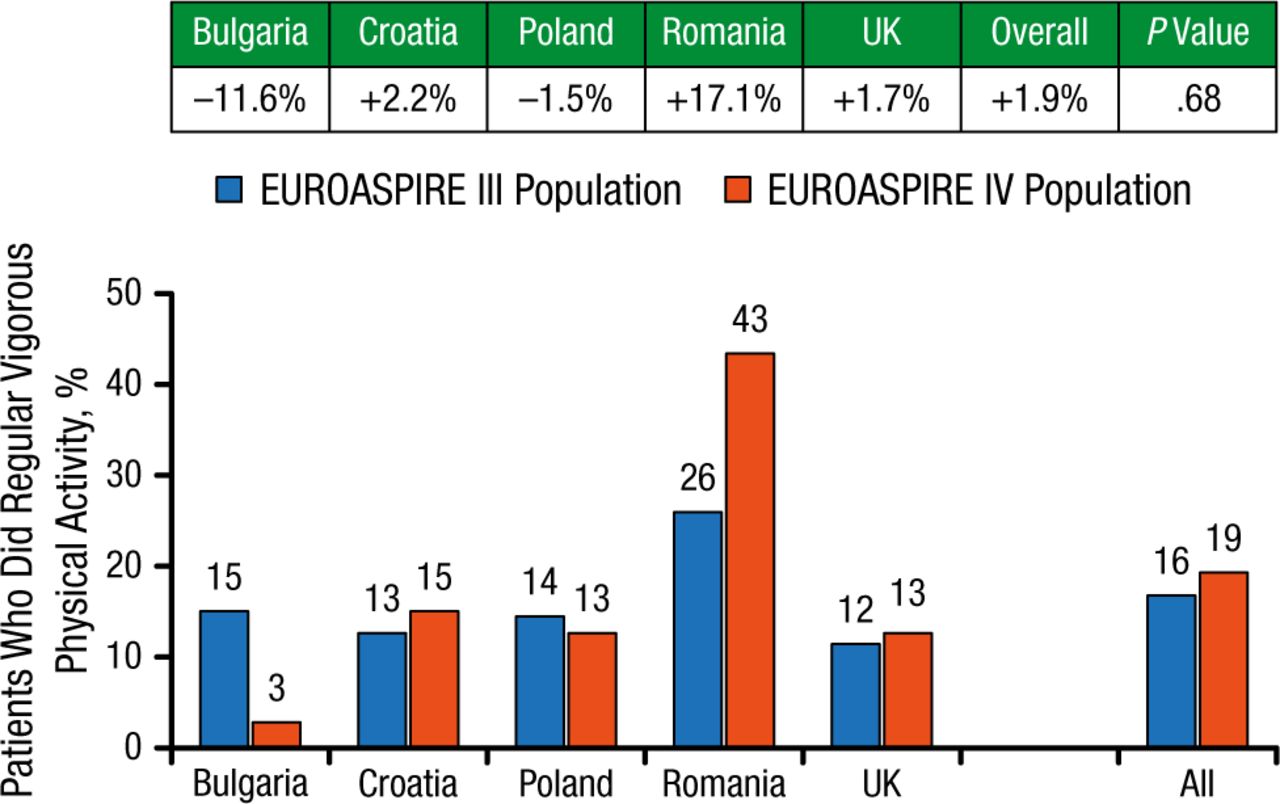
Prevalence of Regular Vigorous Physical Activitya
aVigorous physical activity defined as physical activity outdoors for ≥ 20 min ≥ 3 times a week.
Reproduced with permission from K Kotseva, MD.
Improvements had been made in each country in therapeutic control of blood pressure (28% and 35% in EUROASPIRE III and IV, respectively), total cholesterol (29% and 38% in EUROASPIRE III and IV, respectively), and low-density lipoprotein cholesterol (29% and 37% in EUROASPIRE III and IV, respectively), but there was no significant difference between the 2 surveys for these outcomes. There was no improvement in the glucose control in patients with diabetes mellitus, with glycated hemoglobin being 62% and 60% in EUROASPIRE III and IV, respectively.
The findings indicate the need for lifestyle and medical interventions and a focus on preventive health care that is relevant to the medical and cultural settings in each country.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.