

Summary
Initial data from a randomized trial in patients with treatment-resistant depression show that mindfulness-based cognitive therapy plus medication is significantly more effective than a psychoeducation-based health-enhancement plan plus medication at reducing the severity of depression.
- depression
- mindfulness-based cognitive therapy
- psychoeducation-based health-enhancement program
- treatment-resistant depression
- functional magnetic resonance imaging
- PATH-D study
- cognitive disorders
- psychiatry & psychology clinical trials
Stuart Eisendrath, MD, University of California at San Francisco, San Francisco, California, USA, presented initial data from the PATH-D study [NCT00871299], which investigated whether mindfulness-based cognitive therapy (MBCT) was an efficacious augmentative treatment for reducing symptoms in adults with treatment-resistant depression (TRD). The initial results demonstrated that MBCT improved depressive symptoms in patients with TRD, in association with enhanced regulation of cognitive control areas, as demonstrated by functional magnetic resonance imaging (FMRI).
The study was a single-blind, randomized controlled trial of MBCT plus medication vs a health-enhancement program (HEP) plus medication. Dr Eisendrath explained that the HEP is a psychoeducation-based plan, with an emphasis on physical fitness, agility, nutrition, and music therapy, while MBCT comprises mindfulness meditation with cognitive-behavioral therapy.
One hundred and seventy-three participants were randomized to either the MBCT (n = 87) or the HEP (n = 86) group, for 52 weeks. The primary outcome was percentage reduction in the Hamilton Depression Rating Scale 17-item (HAM-D) score. Inclusion criteria included patients with major depressive disorder with a minimum HAM-D score of ≥ 14 who were currently in medication management. Exclusion criteria included patients with a history of psychotic disorder or substance abuse, as well as those currently using meditation or yoga practice.
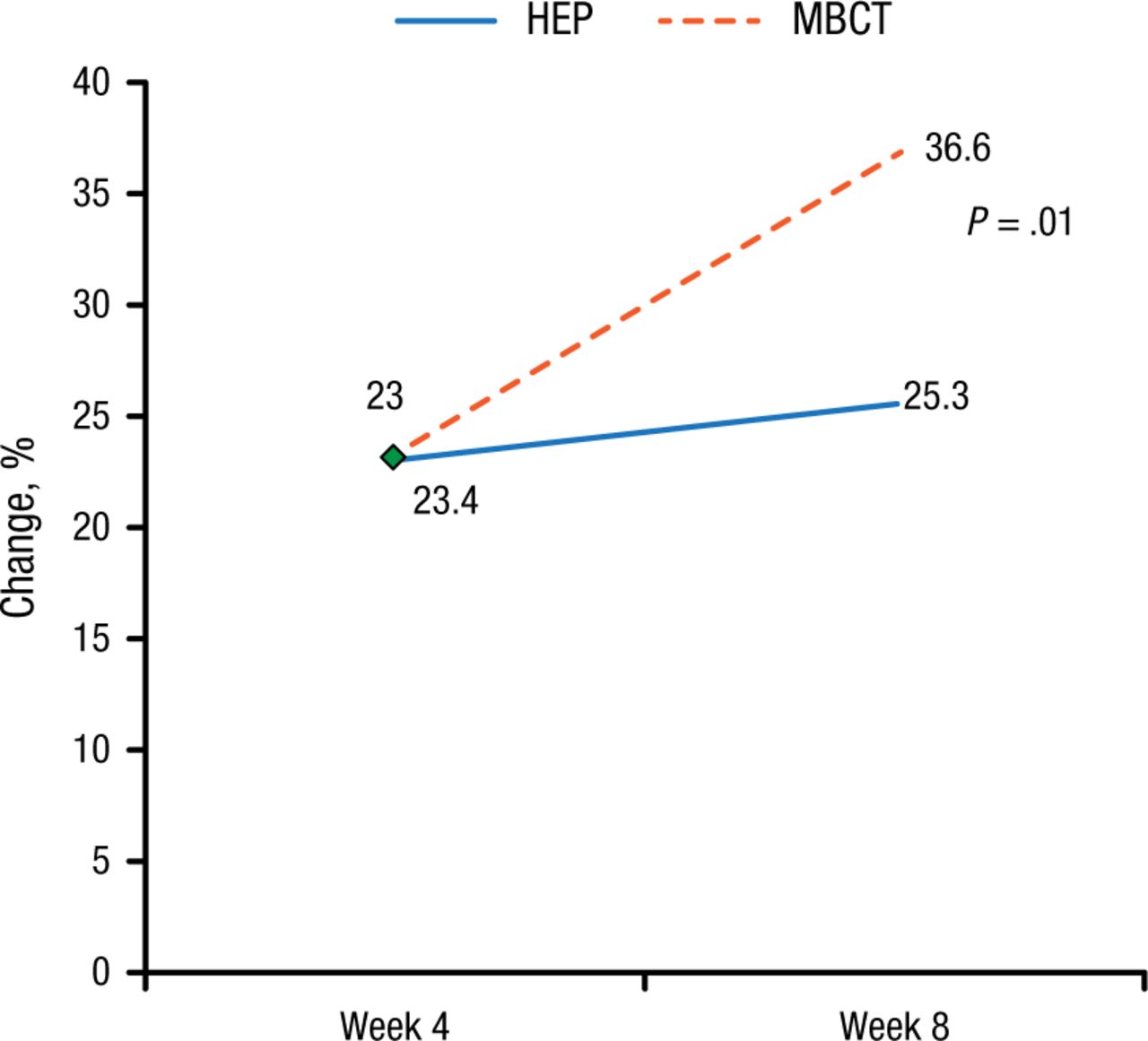
The percentage reduction in the HAM-D score was significantly greater in the MBCT group compared with the HEP group (Figure 1).
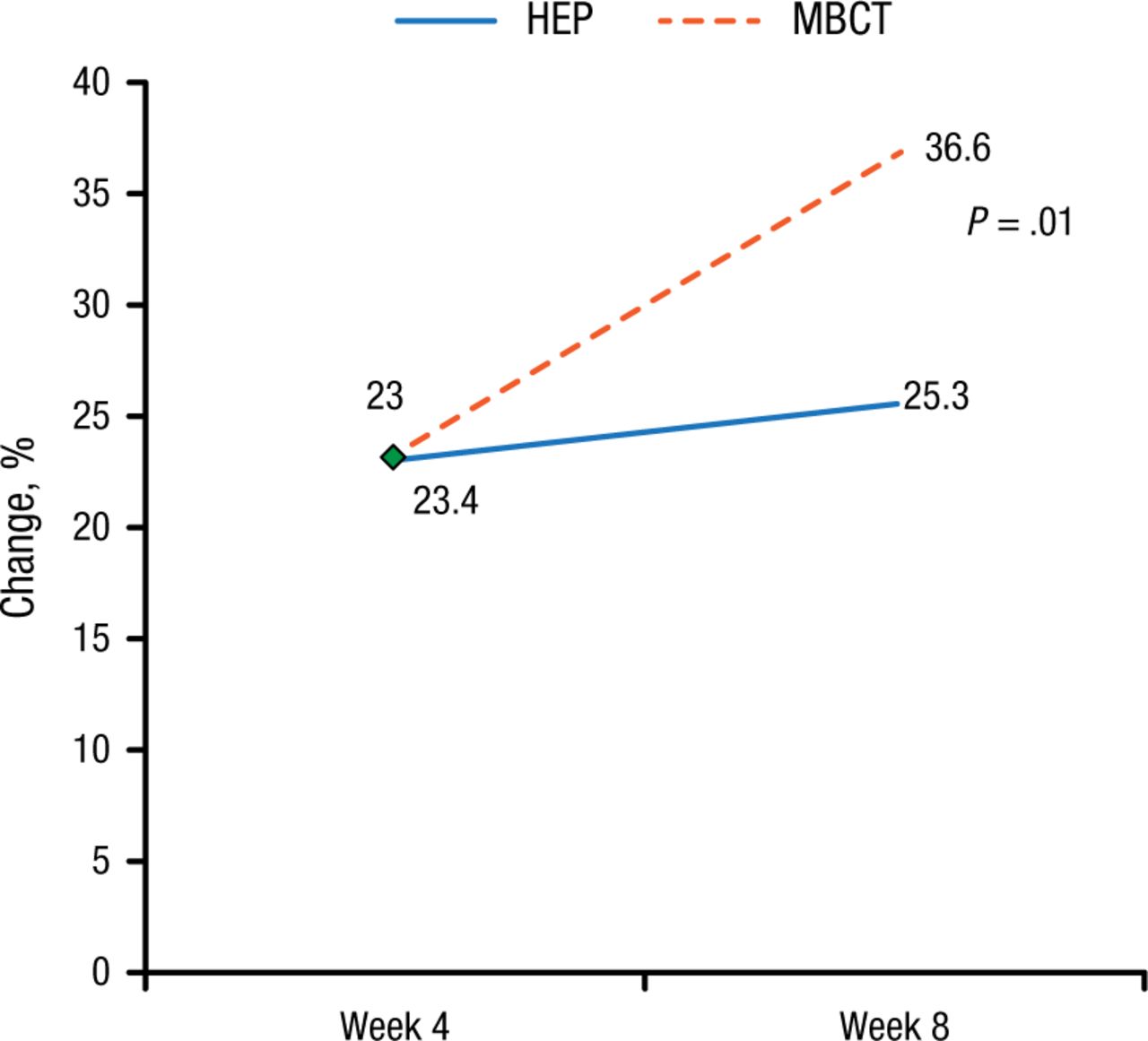
Effect of Treatment on Hamilton Depression Rating Scale Score
HEP, health-enhancement program; MBCT, mindfulness-based cognitive therapy.
Reproduced with permission from S Eisendrath, MD.
A greater percentage of the MBCT group also responded to treatment (29.58% vs 17.19%; P = .0293), as defined by ≥ 50% reduction in HAM-D total score from baseline. However, although treatment remission (defined by a HAM-D total score ≤ 7) was also greater in the MBCT group, it was not statistically significant (21.12% vs 15.63%; P = .1797), which Dr Eisendrath noted was not surprising in the treatment-resistant patient population.
FMRI subset analysis was also performed in the MBCT (n = 44), HEP (n = 44), and healthy control (n = 40) groups. According to Dr Eisendrath, the dorsal executive control center in the brain includes the dorsolateral prefrontal cortex (DLPFC), while the ventral affective processing system includes the ventrolateral prefrontal cortex (VLPFC) and amygdala.
FMRI analysis showed increased VLPFC activation and decreased DLPFC activation in patients with TRD at baseline, suggestive of deficient cognitive control mechanisms in these patients, explained Dr Eisendrath. However, 8 weeks of MBCT, but not HEP, was associated with a reversal of these baseline findings, he added. Improvement in the HAM-D score in the MBCT group was associated with a greater decline in amygdala activation during working memory retrieval compared with baseline (P = .036) and working memory maintenance (P = .05). Overall, these data show that MBCT is associated with activation of cognitive control areas and decreased activation of the affective processing areas, concluded Dr Eisendrath.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.