

Summary
New treatments and clinical information were described for autism spectrum disorders, schizophrenia, anxiety in the transition to young adulthood, mood disorders, and personality disorders. The discussion included connecting genes to behaviors and new therapeutic approaches, along with added understanding of environmental influences and through big data analytics.
- autism spectrum disorders
- schizophrenia
- anxiety
- behavior problems
- mood disorders
- personality disorder
- borderline personality disorder
- adolescents
- family history
- genetic
- bipolar disorder
- social functioning
- anxiety disorders
- psychiatry & psychology clinical trials
A panel of speakers described new treatments and clinical information for autism spectrum disorders (ASDs), schizophrenia, managing anxiety in the transition to young adulthood, mood disorders, and personality disorders.
Toward New Treatments in Autism Spectrum Disorders
Jeremy Veenstra-VanderWeele, MD, Columbia University, New York State Psychiatric Institute, New York, New York, USA, said that ASD is very heterogeneous, with many presentations and patterns existing. Genetic data favor a model where multiple common risk factors come together to lead to convergent risk. The risk factors in ASD are not yet understood, though around 30 genes have been identified as contributing to risk, and about 200 are expected to be identified in the next year. Risk genes feed a cascade of impact from proteins through to behavioral domains.
Early intensive behavioral/developmental interventions and cognitive behavioral therapy (CBT) for anxiety are supported by evidence of moderate strength, while evidence is mixed for social skills training. Most children with ASD should be spending most of their time in behavioral interventions, stated Dr Veenstra-VanderWeele. Evidence is significant that these behavioral interventions improve IQ, language function, and adaptive behavior, but they do not necessarily treat the core diagnosis.
The antipsychotics risperidone and aripiprazole have high strength of evidence, their primary target symptoms are irritability and agitation, and they have significant benefit for hyperactivity/defiance and stereotyped behavior, but their side effects are significant. Attention-deficit/hyperactivity disorder (ADHD) medications treat ADHD in ASD, but the ASD population experiences more side effects and less benefit than the non-ASD population. Selective serotonin-reuptake inhibitors have inconclusive evidence for children with ASD because children have dose-limiting activation, leading them to stop sleeping and become more impulsive.
Treatments that benefit the majority of children with autism are likely to be focused on symptoms and not pathophysiology. These are unlikely to be “cures.” The ultimate goal is to combine medical and behavioral treatment, as drugs by themselves will not rescue ASD.
From Genes to Mechanisms of Illness in Schizophrenia
The big questions in psychiatry research today are how genes and the environment contribute to risk for mental illness and how new targets for the next generation of therapies will be found and validated, said Daniel R. Weinberger, MD, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA. Most risk for psychiatric illness is related to inheritance, and genes transcend phenomenological diagnosis and represent mechanisms of disease. Genes clarify the environment, identify at-risk individuals, and identify biological pathways to develop new treatments.
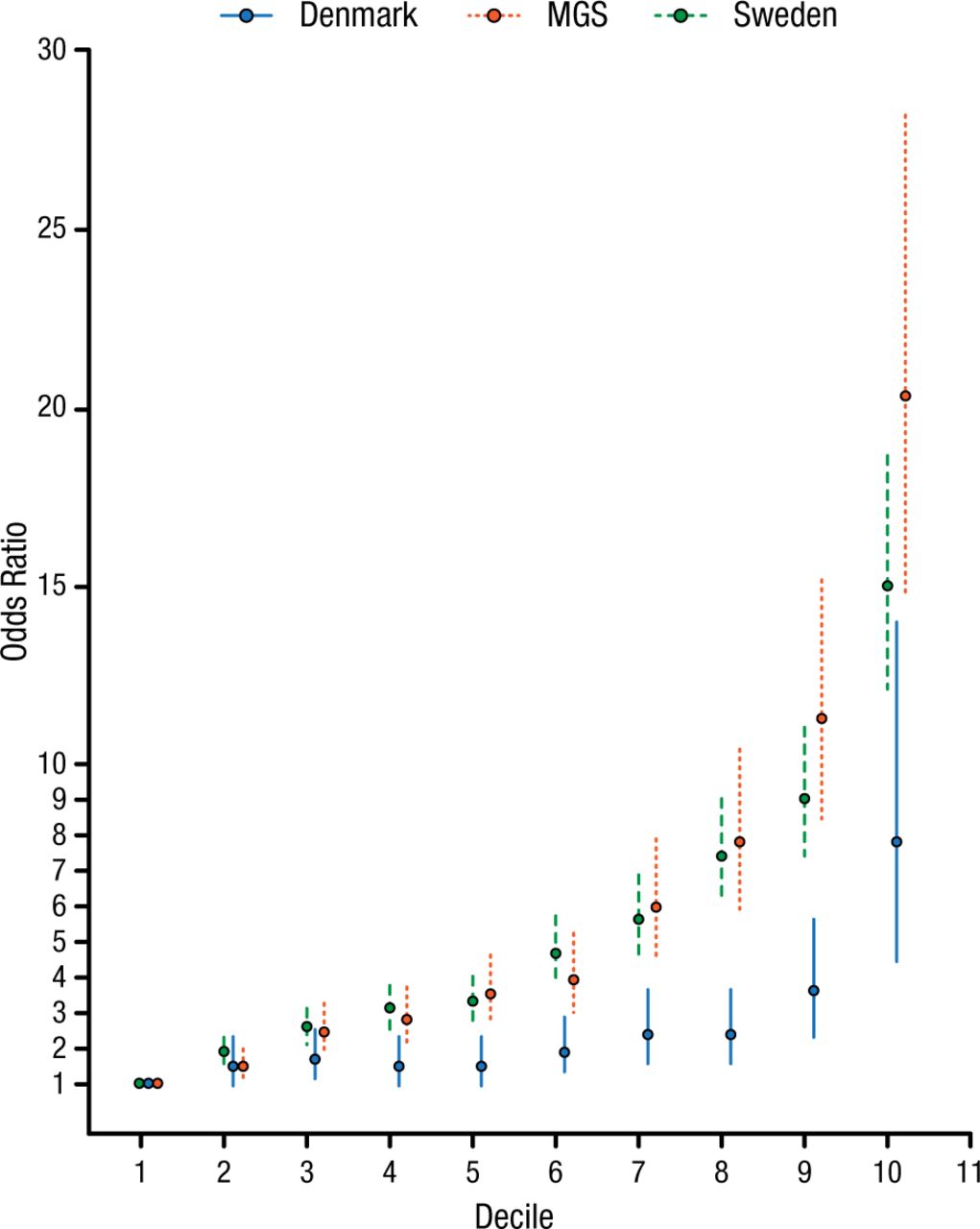
A massive multistage schizophrenia genomewide association study identified 108 significant loci [Schizophrenia Working Group of the Psychiatric Genomics Consortium. Nature. 2014]. These genes include some current drug targets, glutamatergic transmission, neuronal calcium signaling, neuronal ion channels, and neuroplasticity and neurodevelopment. However, these genes individually account for very small increments in risk, and so the odds of developing schizophrenia scale with an increasing risk profile score (Figure 1). This is a meaningful risk factor, though still not adequate to make a diagnosis.
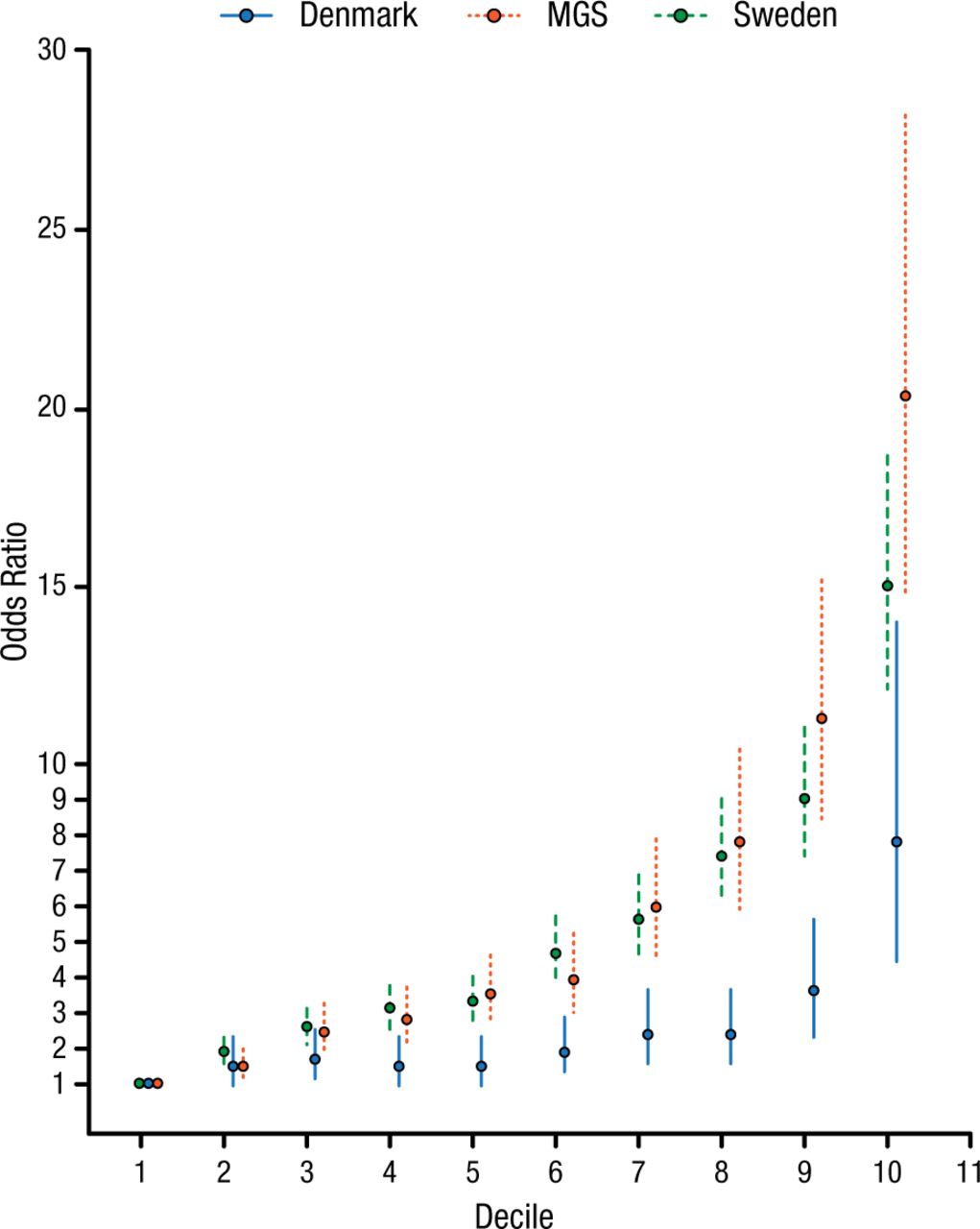
Odds of Developing Schizophrenia Scale With Increasing Risk Profile Score
MGS, Molecular Genetics of Schizophrenia.
Adapted by permission from Macmillan Publishers Ltd: Nature. Schizophrenia Working Group of the Psychiatric Genomics Consortium. Biological insights from 108 schizophrenia-associated genetic loci. 2014;511:421-427, copyright (2014).
Errors in human chromosomes can also be factors in schizophrenia, such as 22q11 hemideletion syndrome, or velo-cardio-facial syndrome, which is found in about 0.5% of patients with the diagnosis of schizophrenia. Yet current understanding can account for the genetic origins of only 20% to 25% of patients with the diagnosis of schizophrenia. The missing genetic risk may be explained by gene interactions that lead to weak individual locus effects and that resist purifying selection. Also, genes interact with the environment to modify the expression of their individual effects, which can lead to exaggerated, compensated, or novel effects. Environment can matter in schizophrenia in regard to such diverse factors as in utero adversity, obstetric complications, socioeconomic circumstances, developmental stress, cannabis, and inflammation.
Managing Anxiety in the Transition to Young Adulthood
Anxiety is highly prevalent, affects 10% to 20% of youth, and is the most common psychiatric condition among children and adolescents, stated Anne Marie Albano, PhD, Columbia University Clinic for Anxiety and Related Disorders, New York, New York, USA. She added that emerging adults, aged 18 to 28 years, have been neglected by the field of psychiatrics.
Symptom improvement tends to be the focus of trials and clinical practice regarding anxiety, but functional outcomes and developmental trajectories have been neglected. The family is a huge factor, and it is not addressed by CBT or medication. Parents get drawn into the cycle of anxiety and overprotect and overcontrol, affecting their child’s developmental milestones. Parents tend to minimize anxiety in the short term, but their efforts solidify the anxiety over the long term.
Clinicians need to attend to symptoms, development, and also parents. Parents may be coaching their children in unconstructive ways instead of problem solving. The overprotection trap can set in early and go through the long term, so the family system must be addressed early. Developmental milestones need to be considered, including those that occur around the time of college and shortly afterward as emerging adults.
Treatment rates are low for anxiety disorders and substance abuse disorders in those aged 19 to 25 years [Blanco C et al. Arch Gen Psychiatry. 2008], and, when mood disorders and drinking behavior combine, suicide attempts increase. Social phobia in young adults aged 17 to 28 years is most predictive of living at home, and these young adults tend to be unemployed and fully financially dependent, according to data from Dr Albano’s clinic.
The Launching Emerging Adults Program (LEAP) manages anxiety and addresses parental overprotection. Context is very important, both family and social context. LEAP adds parent-patient transition sessions that focus on developmental tasks and the parents’ own ideas, beliefs, and fears about their children. Letting the child struggle is more difficult for parents, but the family system must change.
Mood Disorders Research: New Opportunities and Treatments
Mood disorders research is on the edge of big data collaboration. Predictive analytics can now use a smartphone to detect a mood episode before it happens, in contrast to when a patient comes to the clinic and is far into the mood episode, explained Andrew A. Nierenberg, MD, Massachusetts General Hospital, Boston, Massachusetts, USA. These analytics allow real-time data of what is actually happening with people instead of relying on self-observation.
Big data includes large registries, patient communities such as Patients Like Me and Big White Wall, and patient-powered research networks such as the Patient Centered Outcomes Research Network (PCORnet). The PCORnet includes the Mood Patient Powered Research Network, whose goal is to transform the lives of people with mood disorders by collaboration, to conduct prospective comparative effectiveness trials embedded within routine care, to collect clinically useful data on patient-reported outcomes and by integrating electronic medical records, and to have at least 50 000 patient-partners nationwide.
Therapeutic apps and websites are a growing field, and include MoodGym from Australia; Pacifica, which is a premanagement tool for mindfulness and CBT; and NowMeansNow, which is for people who are suicidal.
In addition to approved antidepressants, every medication used for bipolar disorder has been repurposed. Ketamine use has risen in the absence of actual data. Riluzole is an amyotrophic lateral sclerosis drug that is under study for mood disorders and is being used off-label for very refractory patients.
Transcranial near-infrared light passes through the skull and stimulates mitochondria to provide photons to cytochrome c oxidase. It is anti-inflammatory and extremely neuroprotective, with initial data showing improvement over time [Schiffer F et al. Behav Brain Funct. 2009].
Another treatment option being explored is low-frequency magnetic stimulation, which is noninvasive, has positive effects on mood disorders, and may also affect the mitochondrial electron transport chain [Rohan ML et al. Biol Psychiatry. 2014].
Peroxisome proliferator-activated receptors (PPARs) and the associated protein, PGC-1 alpha, which is very involved in metabolism, switch genes on and off and are highly neural-protective. The thiazolidinedione antidiabetic drugs stimulate genes to make PPARs. Pioglitazone was associated with improvement in depressive symptoms and reduced cardiometabolic risk in patients with bipolar disorder and metabolic syndrome/insulin resistance [Kemp DE et al. CNS Drugs. 2014].
Advances in Personality Disorders
Connecting all components, from the molecular level to the individual level, is critical in transforming diagnosis of personality disorders, which are prevalent and disabling, said John M. Oldham, MD, The Menninger Clinic, Baylor College of Medicine, Houston, Texas, USA.
The Alternative Personality Disorder Model is in section 3 of the DSM-V. Retaining the DSM-IV classification and placing this alternative model in a separate section of the DSM-V has been criticized as failure to move the science forward [Tyrer P et al. Lancet. 2015]. A diagnosis using this alternative model has a 43% reduction in the number of items to measure in the DSM-V compared with the DSM-IV, said Dr Oldham. The alternative model in the DSM-V converges with both the proposed definition of personality disorder for the International Classification of Diseases 11th Revision (ICD-11) and the research domain criteria of the National Institute of Mental Health.
Personality disorders are at least moderately heritable, and a shared genetic risk factor may exist. One possibility is that the general factor is the core underlying biological vulnerability for personality disorder [Sharp C et al. J Abnorm Psychol. 2015].
The prefrontal cortex of patients with borderline personality disorder (BPD) seems to have pathology and weakness in regard to inhibitory control over the amygdala, which is normally important for downregulating and controlling emotions. BPD patients have a profound incapacity to maintain cooperation and an impaired ability to repair broken cooperation [King-Casas B et al. Science. 2008]. Patients with BPD are often unable to perceive social gestures. Responses of patients with BPD to oxytocin may make them less able to trust [Bartz J et al. Soc Cogn Affect Neurosci. 2011]. The opioid system is also dysregulated in patients with BPD, and emotional regulation may be enhanced by self-injury [Niedtfeld I et al. PLoS One. 2012].
The core treatment for personality disorders is psychotherapy, with pharmacotherapy being adjunctive and symptom-targeted but not a primary treatment, stated Dr Oldham. Practice guidelines for BPD from a number of countries agree on this approach.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.