

Summary
Medical marijuana is currently legal in 23 states plus the District of Columbia. However, there is ongoing controversy about the role of marijuana in treating medical conditions, the addictive potential of medical and recreational marijuana, the best approaches to treating cannabis use disorder, and which clinical end point is most appropriate.
- marijuana
- medical marijuana
- recreational marijuana
- abstinence
- THC
- dronabinol
- nabinol
- cognitive behavioral therapy
- vouchers
- motivational interviewing
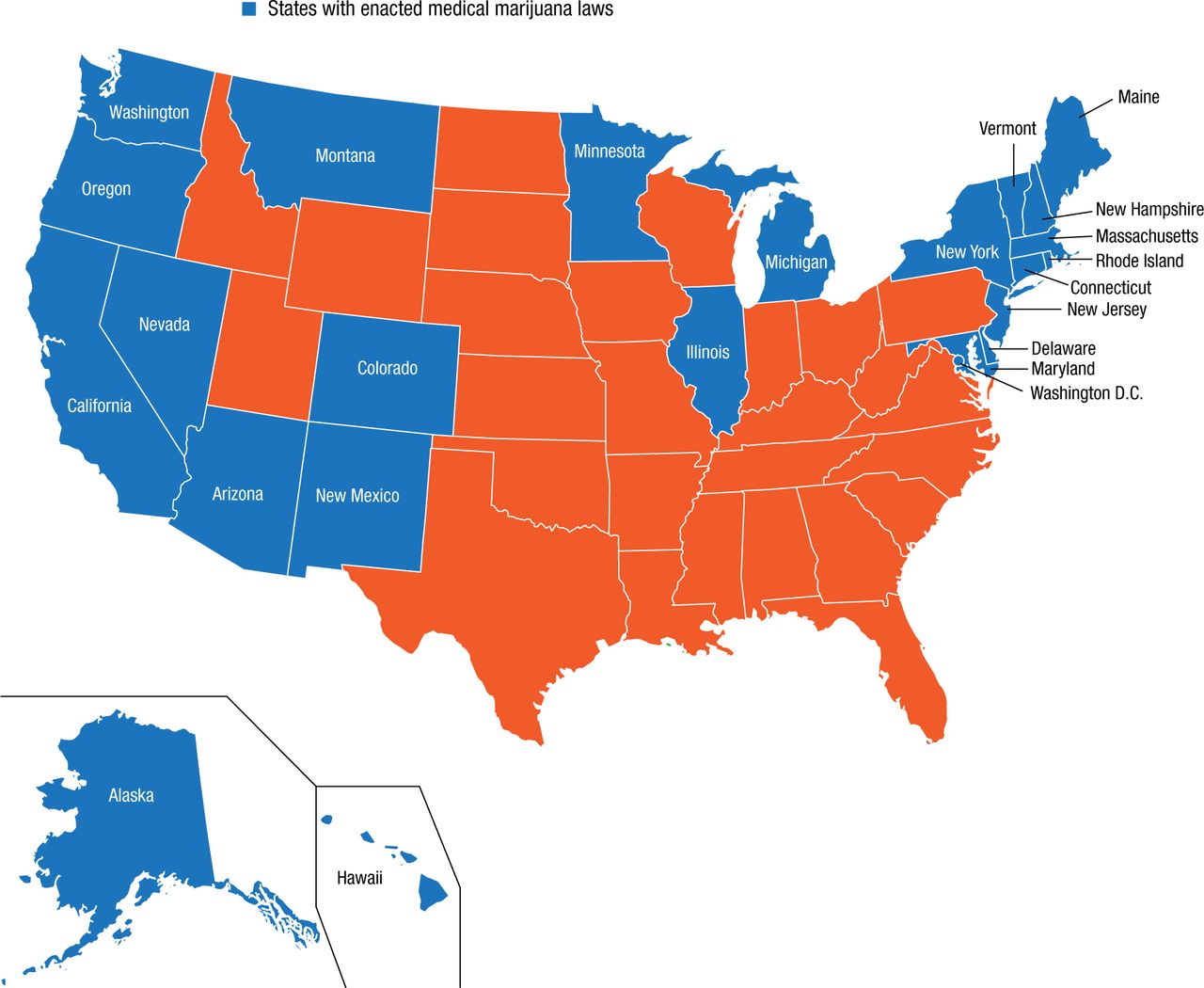
As of April 2015, medical marijuana (MMJ) is legal in 23 states and the District of Columbia (Figure 1). Despite the growing call to expand the use of marijuana for a host of medical conditions, however, the data regarding its safety, effectiveness, and addiction potential are still inconclusive. This session provided a forum for 3 speakers to address the legal and medical issues surrounding the use of recreational marijuana (RMJ) and MMJ.
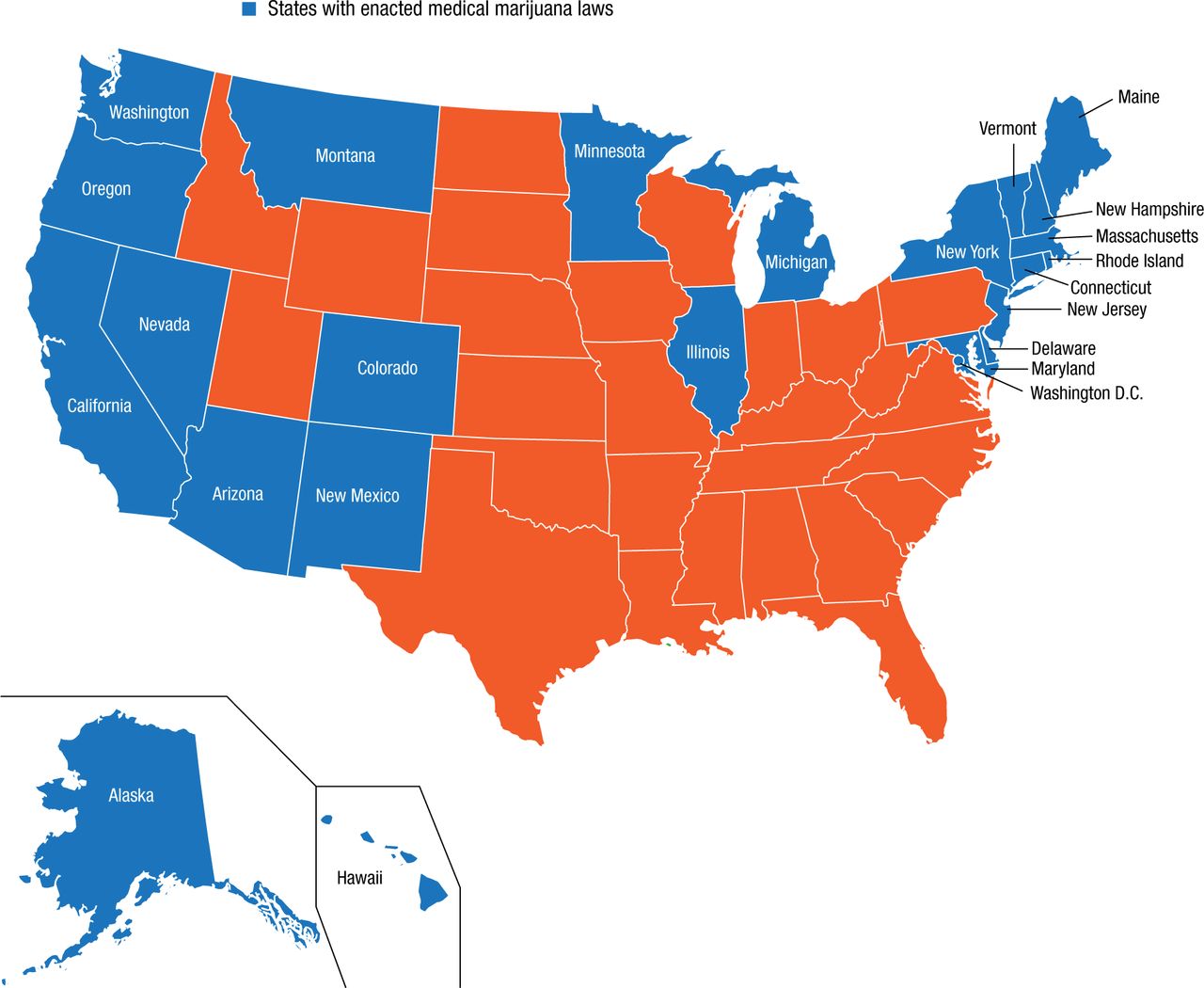
States With Enacted Medical Marijuana Laws
Source: Anthony JC et al. Exp Clin Psychopharmacol. 1994.
Reproduced with permission from KP Hill, MD.
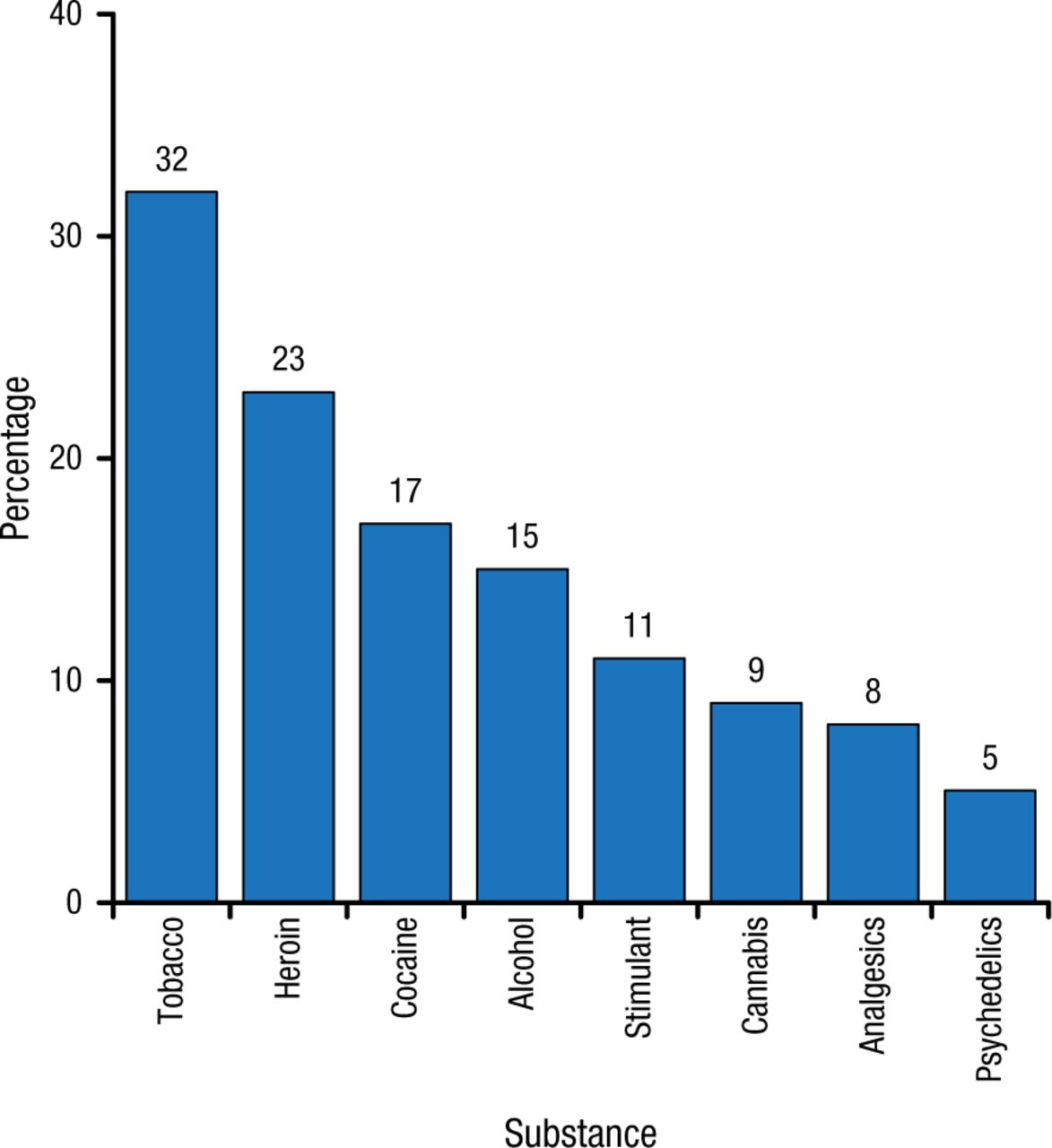
Kevin P. Hill, MD, McLean Hospital, Belmont, Massachusetts, USA, launched the session by discussing the epidemiology of marijuana use and the potential for addiction. According to Dr Hill, almost 20 million Americans used marijuana in the past year, and up to 9% of users may become dependent (Figure 2). Among those who start using in adolescence, 17% may become dependent [Hall W, Degenhardt L. Lancet. 2009].
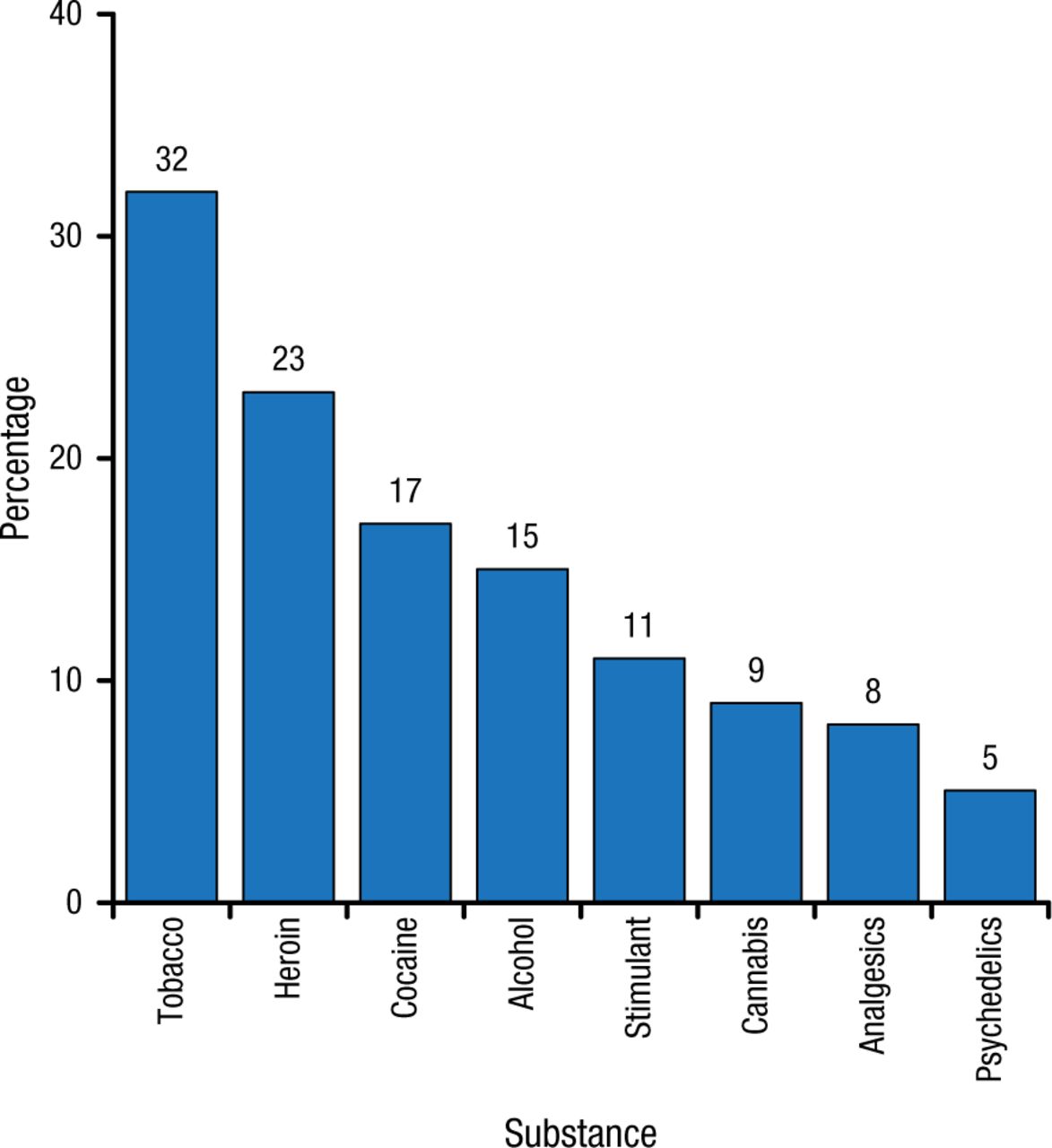
Estimated Prevalence of Dependence Among Users
Source: Anthony JC et al. Exp Clin Psychopharmacol. 1994.
Reproduced with permission from KP Hill, MD.
Dr Hill emphasized that young people who use marijuana regularly can develop neurologic sequelae, including poor cognitive function [Meier MH et al. Proc Natl Acad Sci USA. 2012], increased episodes of anxiety and depression [Crippa GA et al. Hum Psychopharmacol. 2009], and an increased risk of psychotic disorders [Di Forti M et al. Schizophr Bull. 2014]. As well, the symptoms of cannabis withdrawal are similar to those of tobacco withdrawal [Budney AJ et al. J Subst Abuse Treat. 2008].
Each state currently enacts its own MMJ laws, which typically regulate products derived from cannabis leaves, flowers, and roots that are usually sold through state-run dispensaries. These are a different entity than dronabinol (oral tetrahydrocannabinol [THC]) and nabilone, which are medications approved by the FDA for nausea and vomiting associated with chemotherapy and for appetite stimulation in certain wasting illnesses.
Various states have approved cannabis for indications that include cancer, glaucoma, AIDS, hepatitis C, amyotrophic lateral sclerosis, Crohn disease, Parkinson disease, and multiple sclerosis. According to Dr Hill, however, many people who carry MMJ cards do not have one of the above conditions. He also noted that the data linking cannabinoids to symptomatic relief are most robust for chronic pain, neuropathic pain, and spasticity associated with multiple sclerosis [Koppel BS et al. Neurology. 2014]. Dr Hill emphasized that, because state laws often suggest the use of MMJ for medical conditions for which there is little or no scientific evidence supporting the use of MMJ as treatment, the policy is ahead of the science in many states.
Dr Hill closed his presentation with recommendations for patients who ask for MMJ.
Establish a prescribing policy on how you will handle MMJ in your practice.
Be open to evaluating patients who ask for MMJ.
Assess substance abuse risk with a careful medical and psychiatric history.
Psychiatric patients are unlikely candidates for MMJ, so for these patients, MMJ is best recommended by physicians treating the indicated debilitating condition.
Treat a request for MMJ in the same manner as requests for other addictive medications with significant potential side effects, like benzodiazepines or stimulants.
Andrew J. Saxon, MD, University of Washington and VA Puget Sound Health Care System, Seattle, Washington, USA, presented his thoughts on practicing psychiatry in one of the only states where RMJ is legal.
According to Dr Saxon, every producer of RMJ is licensed by the state of Washington and must submit samples of the product to an independent laboratory. Samples are tested for quantities of THC and cannabidiol and for the presence of mold, bacteria, and potentially toxic pesticides and herbicides. If a representative sample does not meet applicable standards, the entire lot must be destroyed.
Washington imposes an excise tax on RMJ, which funds the development of a biennial Healthy Youth Survey, as well as a public information website, substance abuse prevention programs, research programs, care at community health centers, and a cost–benefit analysis. Dr Saxon also reviewed the law regarding driving under the influence (DUI) of marijuana. A blood level ≥ 5 ng/mL of THC 2 hours after a driver is stopped results in a DUI charge. A THC level > 0 with a blood alcohol level ≥ 0.02 ng/mL also results in a DUI charge.
In his work at the Veterans Administration Hospital, Dr Saxon has not seen an increase in either the number of patients or the severity of symptoms associated with cannabis use disorders. He also cited data suggesting that, compared with alcohol, MMJ (a proxy for RMJ) is associated with fewer traffic accidents [Anderson DM et al. J Law Econ. 2013] and that the rate of suicides among men decreased after the legalization of MMJ [Anderson DM et al. Am J Public Health. 2014]. This has reinforced his opinion that, so far, little harm has come from the legalization of high-quality marijuana.
Frances R. Levin, MD, Columbia University Medical College, New York, New York, USA, discussed the growing problem of cannabis use disorders. According to the DSM-V, cannabis use disorder is defined by 11 criteria that include amounts taken, cravings, tolerance, and withdrawal.
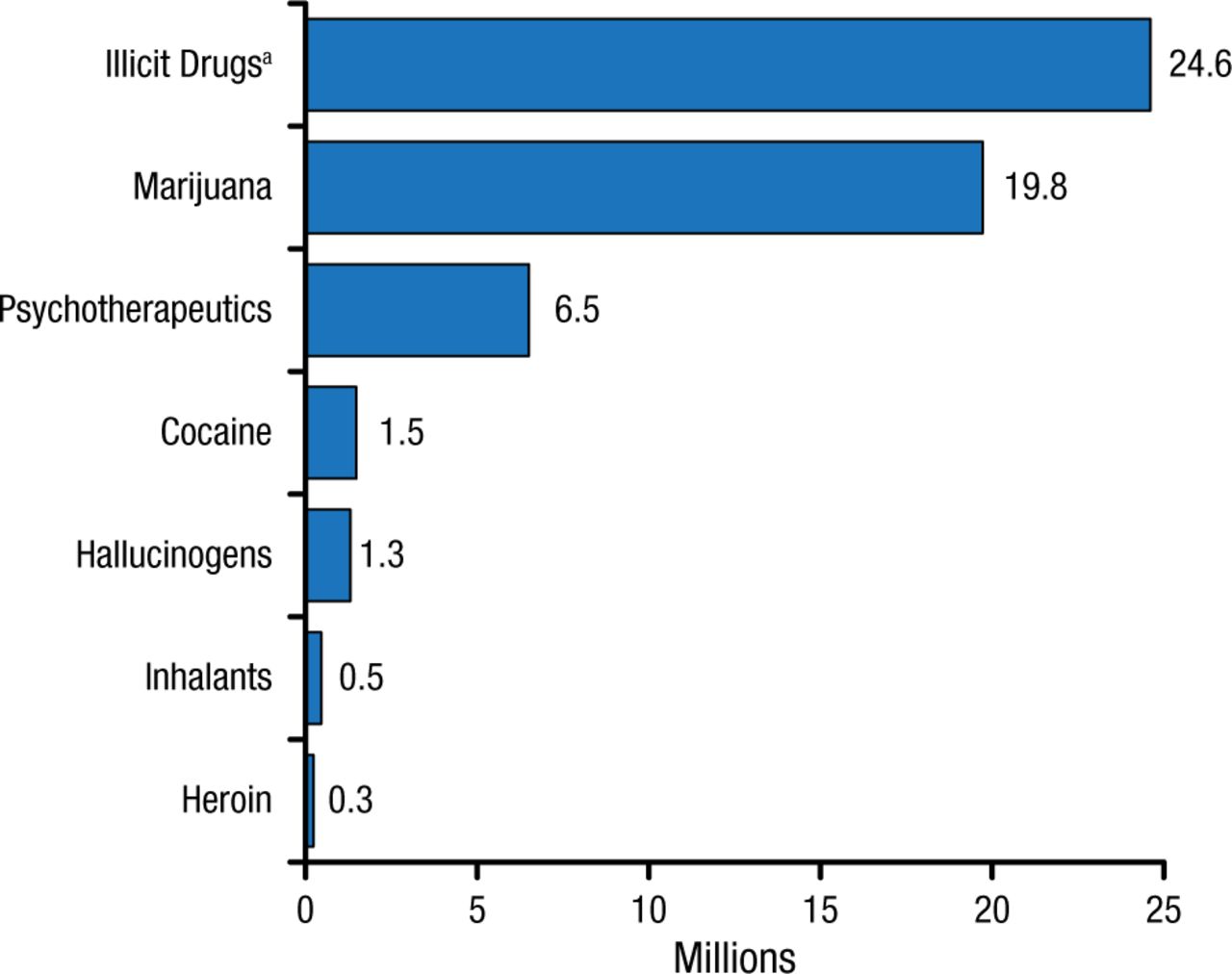
Cannabis is currently the most widely used illicit drug in the United States, with 19.8 million people reporting use in the past month in a 2013 report (Figure 3) [US Department of Health and Human Services. 2013].
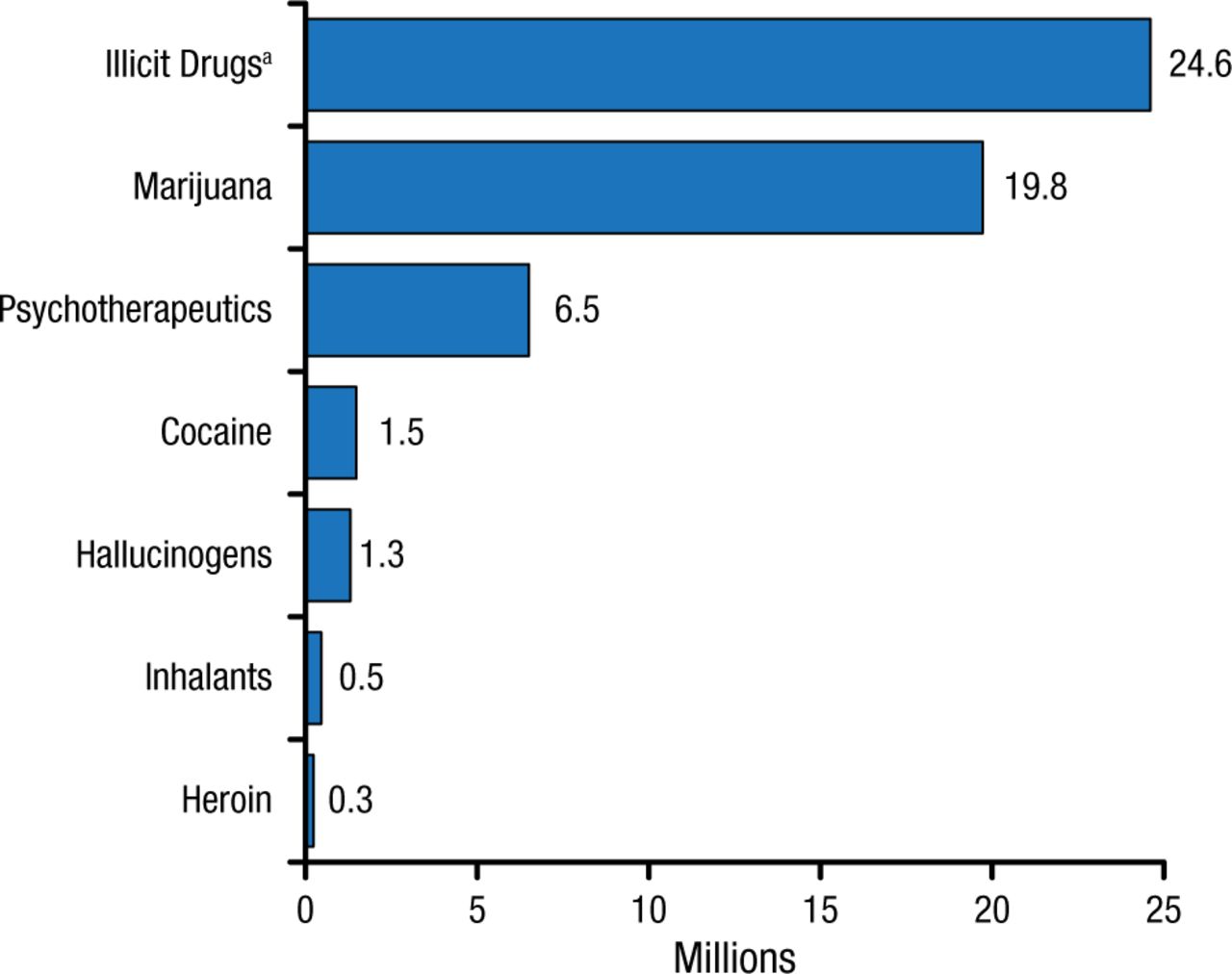
Past-Month Illicit Drug Use Among Persons Aged ≥ 12 y
aIllicit drugs include marijuana/hashish, cocaine (including crack), heroin, hallucinogens, inhalants, and prescription-type psychotherapeutics used nonmedically.
Reprinted from Substance Abuse and Mental Health Services Administration, Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-48, HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.
Psychotherapeutic approaches to cannabis use disorders include motivational interviewing, cognitive-behavioral therapy (CBT), family structural therapy, contingency management strategies, and mindfulness therapy. According to Dr Levin, motivational interviewing is an essential skill for working with substance-dependent patients, as it allows clinicians to talk to patients—especially resistant patients—about substance abuse and supports patients’ self-efficacy [Barnett E et al. Addict Behav. 2012]. The cognitive-behavioral approach to relapse prevention is a flexible approach that introduces and rehearses coping skills to recognize triggers, avoid high-risk situations, cope with cravings, and unlearn maladaptive behavioral skills. Data suggest that this type of treatment is effective in achieving abstinence and reducing marijuana use [Hoch E et al. Eur Neuropsychopharmacol. 2012].
Dr Levin also highlighted a study that combined the use of CBT and abstinence-based vouchers [Budney AJ et al. J Consult Clin Psychol. 2006]. The results suggested that over the first 7 weeks, the vouchers were more successful in promoting abstinence than CBT; over time, however, the vouchers plus CBT had a significantly additive effect compared with either CBT alone or the vouchers alone at 3 months (both P < .05).
For patients who have difficulty reducing or discontinuing their marijuana use, pharmacologic approaches might be indicated. Although a single effective pharmacotherapy has not been identified, the medications or combinations that may be effective include naltrexone [Haney M et al. Neuropsychopharmacology. 2015], gabapentin [Mason BJ et al. Neuropsychopharmacology. 2012], n-acetylcysteine [Gray KM et al. Am J Psychiatry. 2012], and nabilone [Bedi G et al. Addict Biol. 2013].
In closing, Dr Levin urged clinicians to think about a realistic end point for measuring the effectiveness of interventions to reduce marijuana use. Although clinical trials often use continuous abstinence as an outcome measure, Dr Levin suggested that a less stringent measure may be more appropriate.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.