

Summary
The role of global coagulation assays in the clinical setting is unclear. Clinical trials are needed to further assess the relationship between global assays and clinical bleeding. Despite the promise of pharmacogenetics, evidence-based trials are needed to clarify the association between genotype and clinical outcomes, especially related to warfarin.
- pharmacogenetics
- algorithm
- anticoagulation
- warfarin
- assays
- hemophilia
- COX-2
- dabigatran
- clopidogrel
- genomics
- hematology clinical trials
In a session designed to review various aspects of anticoagulation tests and pharmacogenetics, Claude Negrier, MD, PhD, Université Claude Bernard, Lyon, France, began by examining whether global assays can provide useful data in the clinical setting.
He reviewed traditional assays, such as activated partial prothrombin time and prothrombin time, which measure an activity of coagulation factors involved in the intrinsic and extrinsic pathways of coagulation, respectively. These 2 assays are inexpensive, widely used, validated, and typically automated. They can detect coagulation abnormalities and monitor anticoagulation levels in patients who take heparin or warfarin. However, these assays cannot be used to predict thrombotic risk or clinical bleeding phenotype among patients with some inherited bleeding disorders.
In 1 trial [Miller CH et al. J Thromb Haemost. 2013], patients with hemophilia were tested for factor VIII inhibitors through 3 clotting assays: modified Nijmegen-Bethesda Clotting Assay, a chromogenic Bethesda assay, and a novel fluorescence immunoassay—the latter 2 of which were unable to demonstrate factor VIII specificity for 26% of 0.5 to 1.9 Nijmegen-Bethesda units.
Prof Negrier then discussed the challenges in assessing coagulation status in patients with inherited or acquired coagulation disorders. While activated partial prothrombin time and prothrombin time are able to identify hemostatic dysfunction involving the intrinsic, extrinsic, and common pathways of coagulation, they are not useful for assessment of hypercoagulability or fibrinolytic abnormalities. A more global approach to the coagulation system would reflect the complex interactions between the pro- and anticoagulant mechanisms that might better reflect clinical phenotypes and guide therapeutic interventions.
Moving from anticoagulation to pharmacogenetics, Guillaume Paré, MD, McMaster University, Hamilton, Ontario, Canada, reviewed the role of pharmacogenetics in treating arterial disease. He began by discussing the FDA boxed warning on clopidogrel, which recommends that CYP2C19 genotyping be considered prior to the drug’s prescription. A meta-analysis of 32 studies, however, suggested that whereas there was an association between the CYP2C19 genotype and clopidogrel responsiveness, overall there was no significant association of genotype with cardiovascular events [Holmes MV et al. JAMA. 2011].
According to Prof Paré, there is a need for more evidence to determine the benefit of CYP2C19 testing before clopidogrel is prescribed. Because genetic testing has obvious costs and other risks, 1 option is to use an alternative antiplatelet agent such as ticagrelor, which appears to be more effective than standard-dose clopidogrel, irrespective of genotype [Paré G, Eikelboom JW. Circ Cardiovasc Interv. 2011; Wallentin L et al. Lancet. 2010]. He argued that there is no need for genotyping if the alternative treatment is superior to standard care, regardless of genetic results. A case for genotyping can be made if the results will change clinical management depending on genotype.
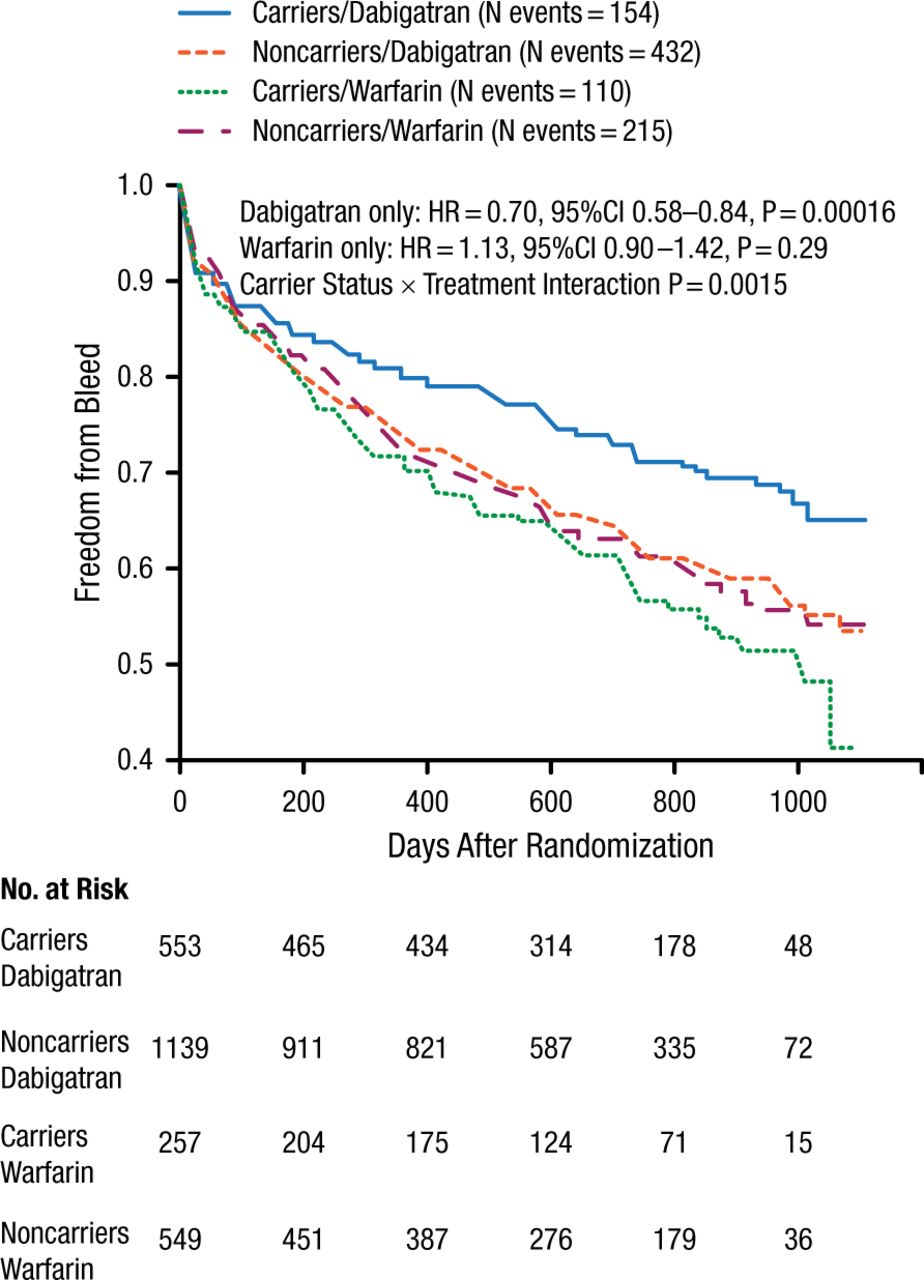
Prof Paré then went on to discuss dabigatran. In the RE-LY trial [Connolly SJ et al. N Engl J Med. 2009], a subsequent genome-wide association analysis identified 32.8% of patients with the minor allele rs2244613 (CES1) [Paré G et al. Circulation. 2013]. This allele was associated with lower exposure to active dabigatran and a lower risk of bleeding as compared with patients who did not carry the allele (Figure 1).
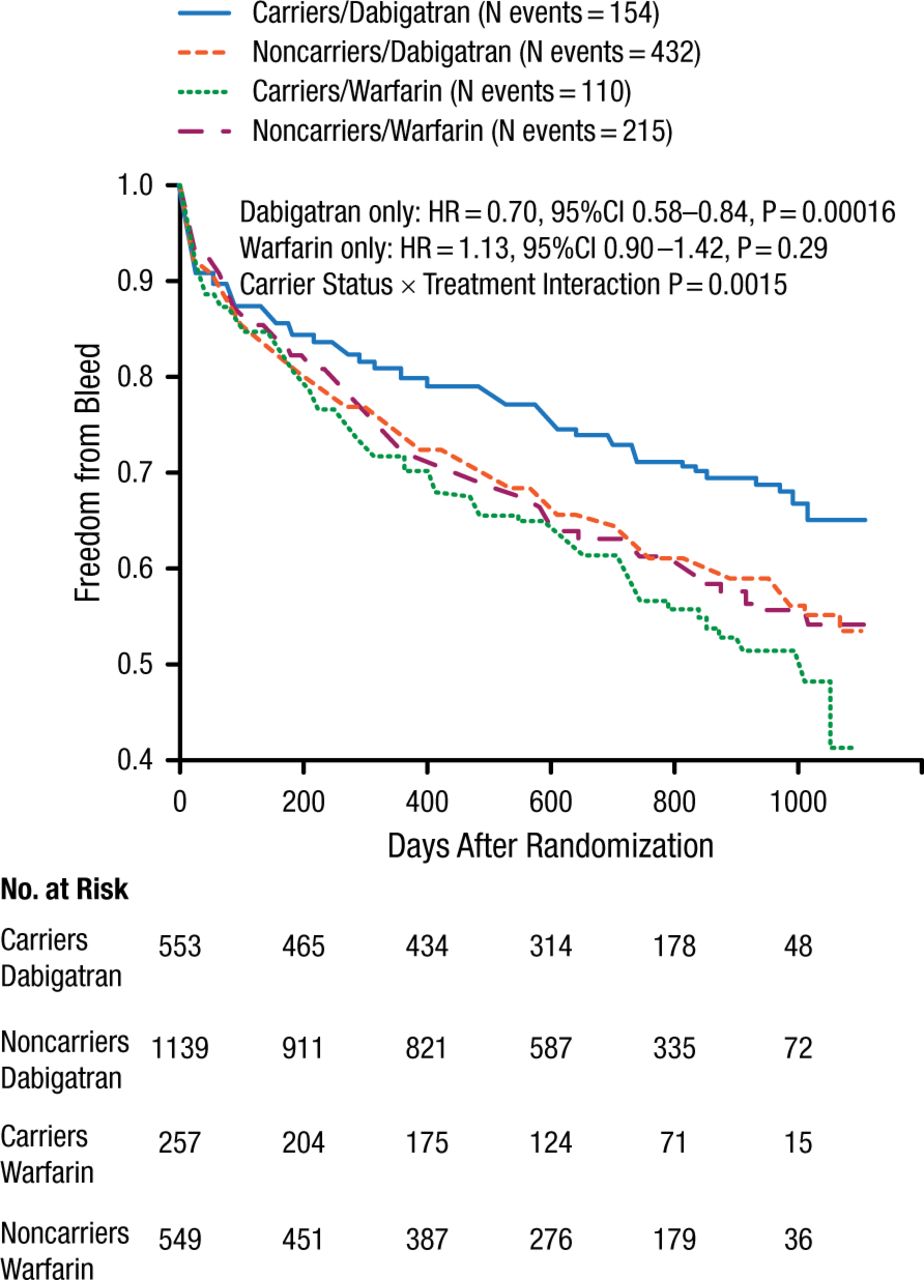
Risk of Bleeding According to rs2244613 Status
Reprinted from Paré G et al, Genetic determinants of dabigatran plasma levels and their relation to bleeding, Circulation, 2013, Vol 127, Issue 13, Pages 1404-12, with permission from American Heart Association, Inc.
Prof Paré then discussed cyclooxygenase-2 activity and the genetic variant rs20417 of the PTGS2 gene. A detailed analysis of almost 50 000 patients showed that the rs20417 variant was associated with a reduced risk of major cardiovascular events, especially in patients who took aspirin [Ross S et al. Eur Heart J. 2014].
In conclusion, Prof Paré emphasized that despite the promise of pharmacogenetics, there is a need for evidence-based recommendations, especially related to clopidogrel. Pharmacogenetic effects can be population specific and possibly even tissue specific, and they must be incorporated into clinical trials.
Stephen E. Kimmel, MD, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA, then discussed genetic approaches to warfarin dosing. One nongenetic approach is to use fixed dosing; a second approach is to use clinical information to adjust the dose; and a third is to incorporate what we know about genetics alongside clinical information. In a validation cohort of 1009 patients from a larger cohort of 4043 patients who took 3 ranges of warfarin, a pharmacogenetic algorithm produced recommendations closer to the required therapeutic dose when compared with a fixed dose of 35 mg/wk or a clinical algorithm [The International Warfarin Pharmacogenetics Consortium. N Engl J Med. 2009]. These predictions were significantly better among patients who took the lowest (≤ 21 mg/wk) and highest (≥ 49 mg/wk) doses (P < .001, both). In these 2 groups, the fixed dose never reached 20% of the actual stable therapeutic dose.
Dr Kimmel then went on to discuss whether pharmacogenetics will improve care of patients on warfarin. Because warfarin is a complex drug that is affected by pharmacokinetics, pharmacodynamics, target proteins, drug-drug interactions, adherence, and diet, it is not clear that pharmacogenetic dosing will improve outcomes. Therefore, research has turned to randomized trials to provide unbiased controlled comparisons of pharmacogenetic-based dosing of warfarin vs other strategies. The comparator group in these trials might include routine clinical care (fixed dose and clinician-determined empiric doses), a clinical algorithm (eg, dose, age, target INR, other medications, sex), or both.
The COAG trial [Kimmel SE et al. N Engl J Med. 2013] compared a pharmacogenetic algorithm with a clinical dosing algorithm in patients on warfarin. At 4 weeks, there was no difference in the mean time that patients spent in therapeutic range. However, among African American patients, the mean percentage of time spent in the therapeutic range was higher in the clinical algorithm than the pharmacogenetic algorithm (P = .03). Dr Kimmel also reviewed a genotype-guided trial suggesting no incremental benefit on anticoagulation control via CYP2CP and VKORC1 to determine initial acenocoumarol or phenprocoumon dosing [Verhoef T et al. N Engl J Med. 2013]. However, a pharmacogenetic algorithm was superior to an approach that incorporated fixed dosing by age instead of a formal clinical algorithm [Pirmohamed M et al. N Engl J Med. 2013].
Dr Kimmel summed up his presentation with additional data from the COAG trial. The pharmacogenetic-guided algorithm was able to predict doses of warfarin within 1 mg/d of maintenance dose compared with a hypothetical 5-mg/d approach, while the clinical-guided strategy appeared to be particularly successful in African American patients (Table 1).
Predicted Dose of Warfarin Within 1 mg/d of Maintenance Dose
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.