

Summary
Alcoholic liver disease is a leading cause of liver-related mortality and is associated with a significant financial burden. The 2010 treatment guidelines recommend corticosteroids and pentoxifylline, although the evidence for their utility is inconsistent. Although controversial, there is a small group of patients who may be candidates for liver transplant.
- alcoholic liver disease
- pentoxifylline
- corticosteroids
- transplant
- prednisolone
- abstention
- liver transplant
- model for end-stage liver disease
- alcoholic hepatitis
- gastroenterology guidelines
Alcoholic liver disease (ALD) is a major cause of liver disease in Western countries [Bruha R et al. World J Hepatol. 2012] and is among the leading causes of cirrhosis and liver-related death worldwide [Frazier TH. Therap Adv Gastroenterol. 2011]. In his state-of-the-art lecture, Vijay Shah, MD, Mayo Clinic, Rochester, Minnesota, USA, presented a comprehensive review of recent research regarding ALD, with a focus on alcoholic hepatitis (AH).
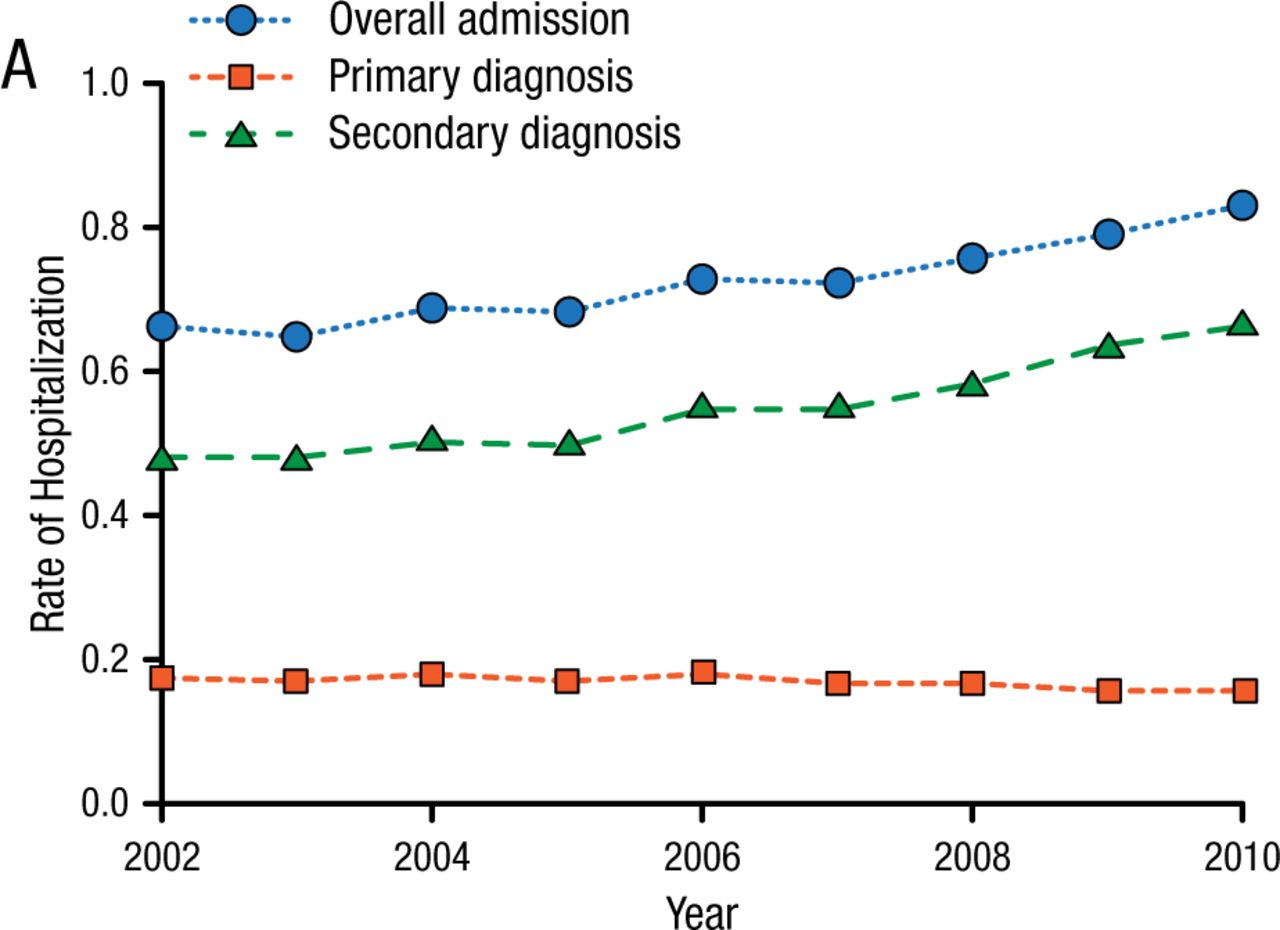
Dr Shah began by highlighting the costs of AH. Over the past 10 years, hospital admissions for AH-related conditions have continued to increase, especially for secondary complications related to AH such as sepsis, acute renal failure, and gastrointestinal bleeding (Figure 1) [Jinjuvadia R et al. J Clin Gastroenterol. 2014]. Ten years ago, hospital costs were estimated to be approximately $25 000 per hospital admission for AH; today, they are estimated to be $40 000 per admission.
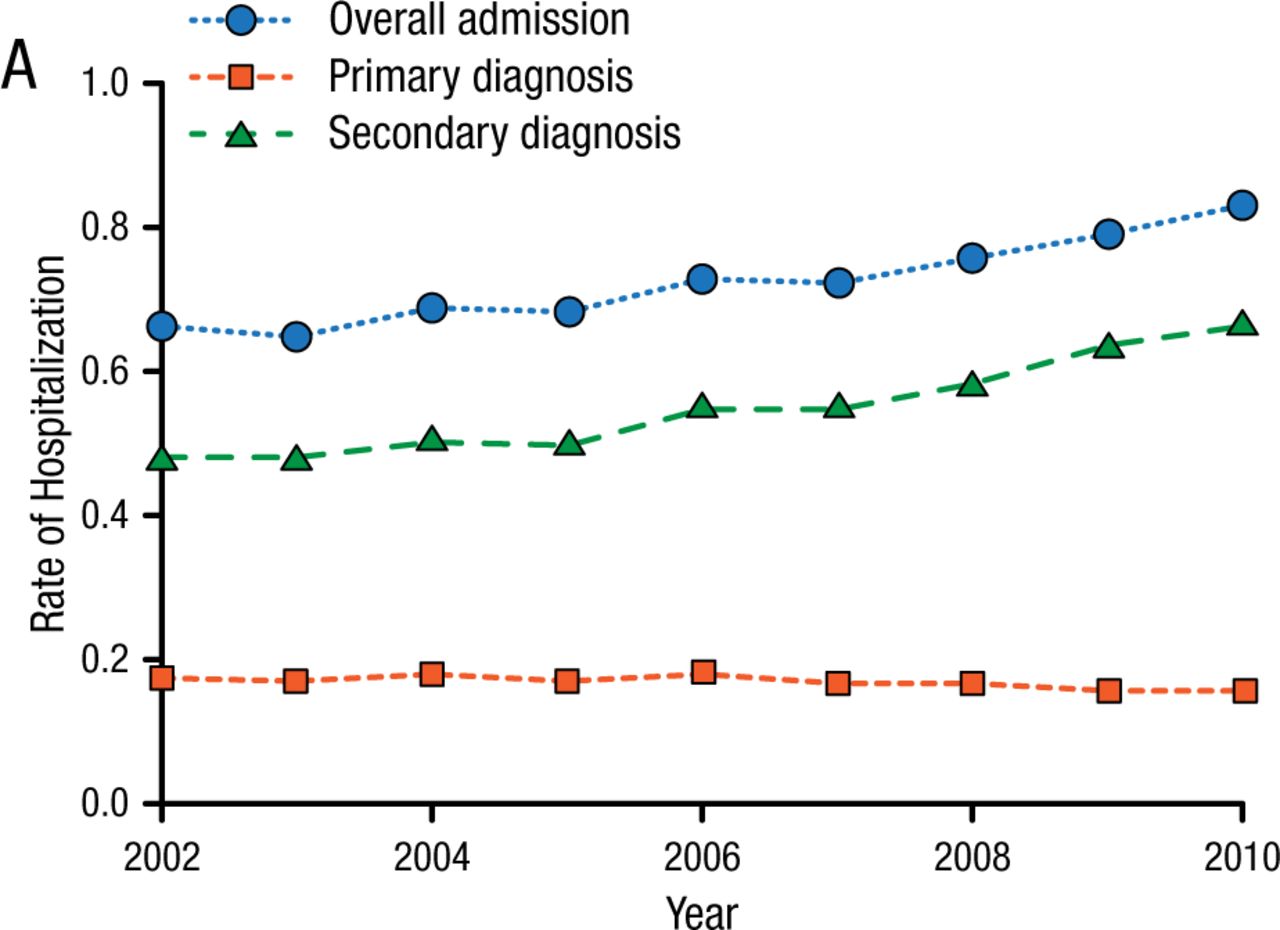
Increases in Alcoholic Hepatitis Hospitalization Rates in the United States, 2002-2010Rate of hospitalization for the diagnosis of alcoholic hepatitis (AH) in the United States from 2002 to 2010.
Reprinted from Jinjuvadia R et al. Trends in Alcoholic Hepatitis-related Hospitalizations, Financial Burden, and Mortality in the United States. J Clin Gastroenterol. Published online ahead of print 2014 (doi: 10.1097/MCG.0000000000000161). With permission from Lippincott Williams & Wilkins.
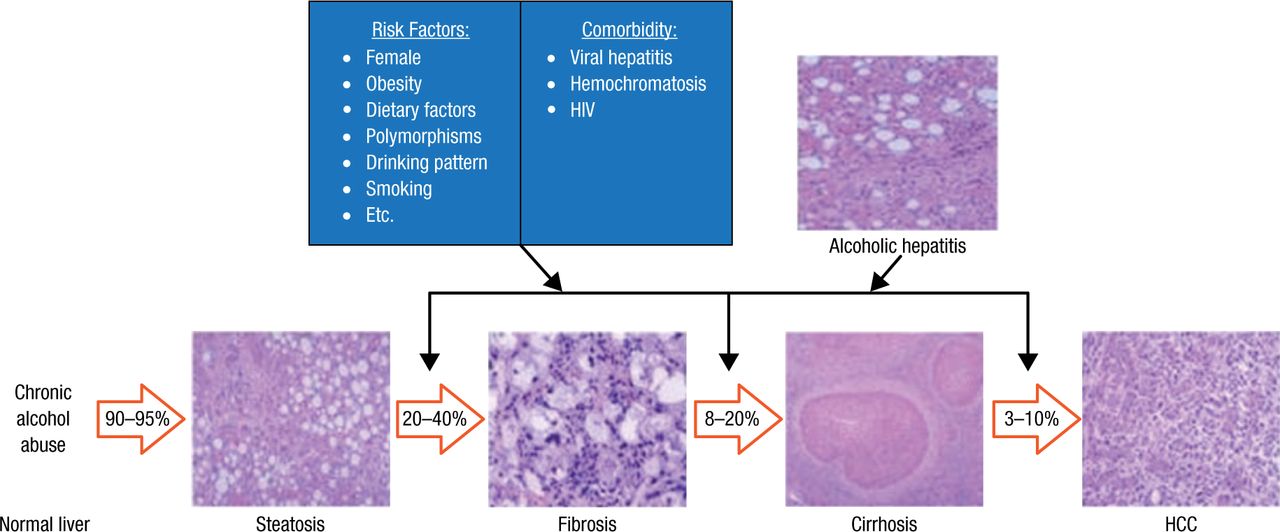
According to Dr Shah, the increased utilization of liver transplantation for patients with ALD is also associated with increased costs, as the percentage of these patients undergoing liver transplantation will likely increase as the number of patients with hepatitis C decreases [Wong RJ et al. Gastroenterology. 2015]. Dr Shah then went on to discuss the risk factors and comorbidities associated with the progression of ALD (Figure 2) [Gao B, Bataller R. Gastroenterology. 2011].
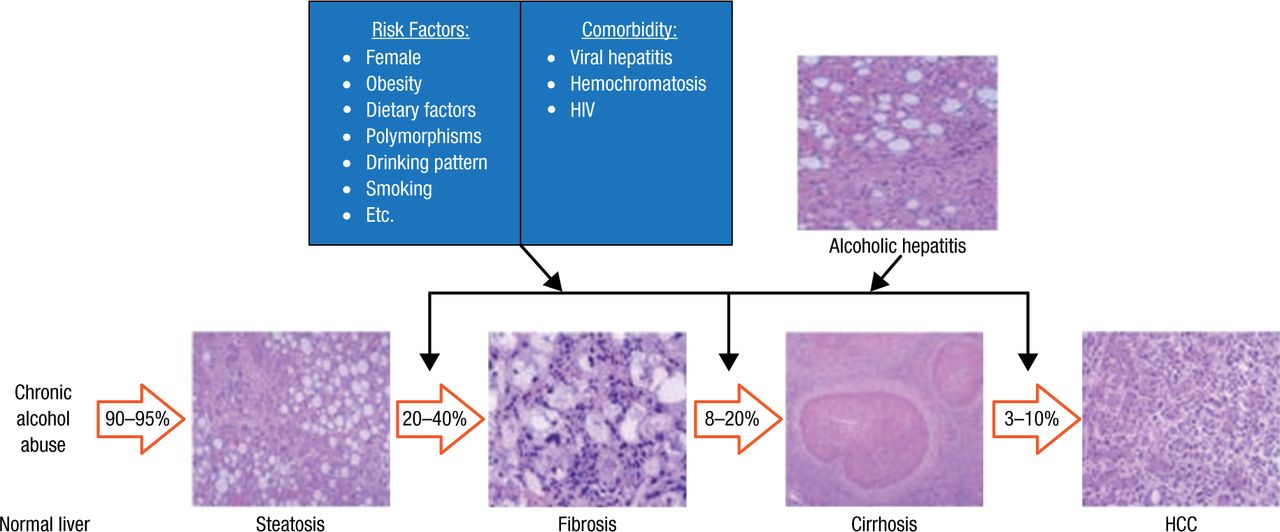
Histopathological Progression and Risk Factors of ALD
Spectrum of ALD, risk factors, and comorbidity. More than 95% of heavy drinkers develop fatty liver, but only up to 35% of this population develops more severe forms of ALD, including fibrosis, alcoholic hepatitis, cirrhosis, and HCC. Many risk factors have been proposed for the severe forms of ALD. Alcohol consumption and comorbid factors act in synergy to accelerate the progression of ALD.
Reprinted from Gastroenterology, Vol. 141, Gao B et al, Alcoholic Liver Disease: Pathogenesis and New Therapeutic Targets, Pages No. 1572-1585, Copyright (2011), with permission from AGA Institute.
In discussing the diagnosis of AH, Dr Shah highlighted the ongoing controversy regarding the value of liver biopsy. An accurate diagnosis can guide treatment, as alternative diagnoses have different therapies and the therapy for AH can be toxic to patients with a different type of liver disease. On the negative side, liver biopsies are expensive, may be difficult to distinguish from other etiologies of hepatitis, and can result in serious complications, especially in patients with comorbid coagulopathy and renal insufficiency. According to Dr Shah, tools such as breath biosensors [Hanouneh IA et al. Clin Gastroenterol Hepatol. 2014] and the Alcoholic/Nonalcoholic Steatohepatitis Index [Dunn W et al. Gastroenterology. 2006] may eventually offer sufficient diagnostic accuracy such that a clinician will need to order a liver biopsy only 15% to 20% of the time.
Dr Shah also reviewed some metrics to determine whether a patient with AH will respond to steroids, such as an early change in bilirubin levels, the Lille score, and the model for end-stage liver disease (MELD) score. New data suggest that a combination of the MELD score and the Lille score provides the optimal prognostic scoring system [Louvet A et al. Gastroenterology. 2015]. He then moved on to highlight the systemic inflammatory response syndrome, which can predict multiorgan failure and mortality in patients with AH using blood-based markers such as levels of procalcitonin, C-reactive protein, and lipopolysaccharide [Michelena J et al. Hepatology. 2015].
The remainder of the presentation focused on treatment approaches. According to Dr Shah, pharmacotherapy influences survival by only 1 month; 6-month survival is most influenced by abstinence from alcohol and appropriate nutrition status. The complications of cirrhosis will have the greatest influence on survival by 12 months. While abstinence is a key driver of survival, pharmacologic options for alcohol addiction include baclofen [Yamini D et al. Alcohol Alcohol. 2014] and acamprosate. It is important to note that baclofen is not FDA approved for patients with ALD [Vuittonet CL et al. Am J Health Syst Pharm. 2014] and acamprosate is approved for a Child–Pugh score of A or B only.
When it comes to treating patients, there appears to be a discrepancy between treatment guidelines and clinical practice. Clinical guidelines recommend the use of prednisolone for patients with severe disease and no contraindications to steroids; these same patients could also be considered for pentoxifylline instead of prednisolone [O’Shea RS et al. Hepatology. 2010]. However, survey data suggest that < 50% of gastroenterologists prefer using corticosteroids to treat patients with ALD, and less than one-third preferred pentoxifylline [Singal AK et al. World J Gastrointest Pharmacol Ther. 2013].
Outcomes from treatment trials of patients with AH have been inconsistent. The recently published STOPAH trial [Thursz MR et al. N Engl J Med. 2015] suggested that in patients with AH, neither pentoxifylline nor prednisolone was associated with a significant reduction in 28-day mortality. In addition, there was no improvement in outcomes at 90 days or 1 year. However, a recent meta-analysis of 22 trials presented by Singh and colleagues at Digestive Disease Week 2015 suggested that both corticosteroids and pentoxifylline decreased short-term mortality. No intervention was able to decrease medium-term mortality. Pentoxifylline decreased the risk of acute kidney injury, and no intervention—including corticosteroids—increased the risk of infection. Other studies have suggested that prednisolone was more beneficial than pentoxifylline over 30 days, although no difference was noted in survival between the 2 groups at 180 days in 121 patients with severe AH [Park SH et al. J Hepatol. 2014], and that combination therapy with corticosteroids and pentoxifylline was not superior to corticosteroid monotherapy at 6 months in patients with severe AH [Mathurin P et al. JAMA. 2013]. He also described a new blood biomarker that can be used to determine which patients are most likely to respond to corticosteroids [Dhanda AD. Hepatology. 2015].
Dr Shah closed his presentation with a discussion regarding the benefit of liver transplantation for patients with AH. While liver transplantation is the definitive cure for liver disease, only a few patients with AH are candidates for this procedure. At least one study has shown that early liver transplantation can improve survival in patients with a first episode of severe AH not responding to medical therapy after 1 week [Mathurin P et al. N Engl J Med. 2011].
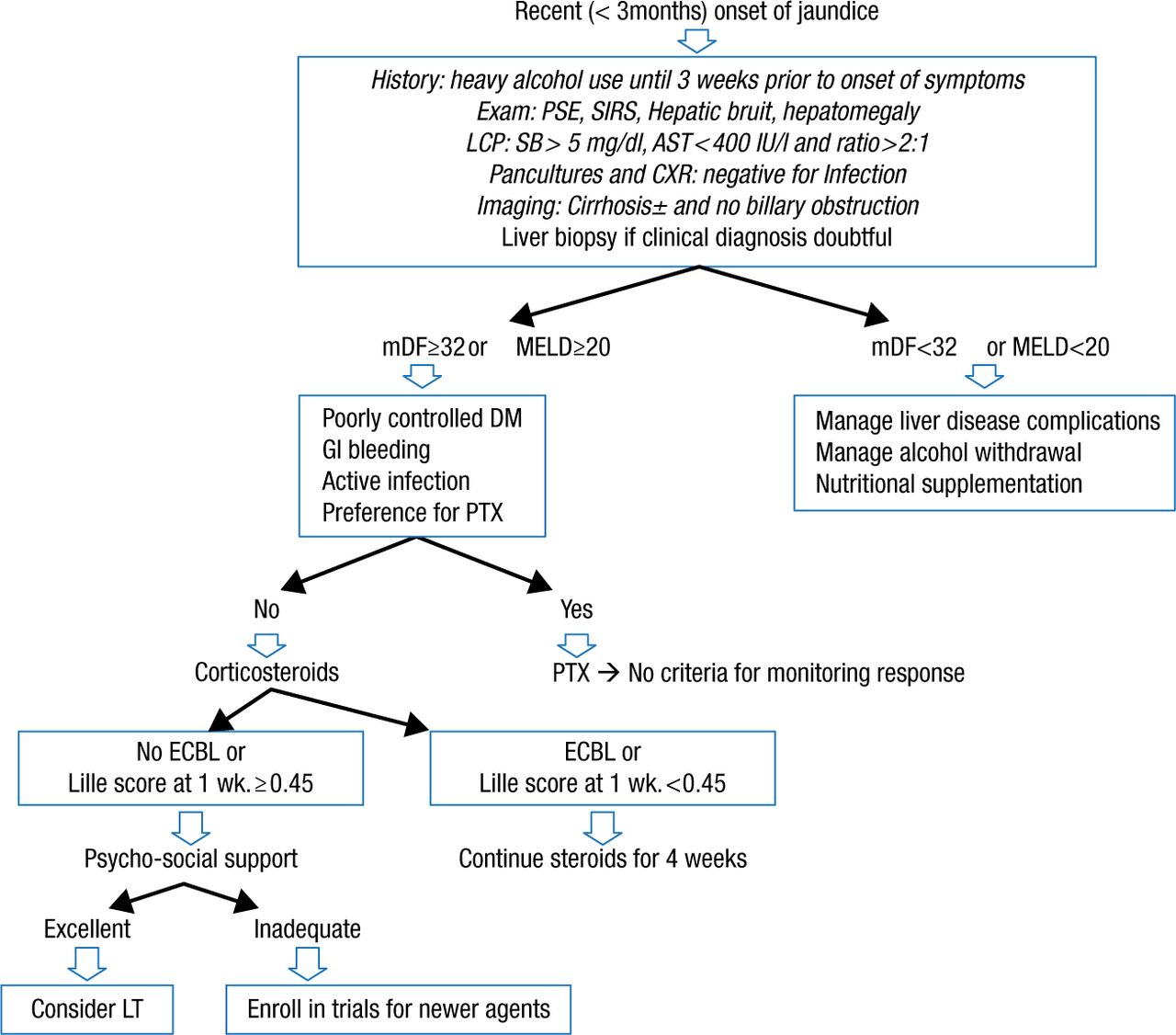
According to Dr Shah, the key to successful outcome following a liver transplant is in selecting appropriate patients to undergo the surgery. Most patients are required to abstain from alcohol for 6 months before being listed for transplant. However, most patients with severe AH are not likely to live for 6 additional months. Therefore, a very small percentage of patients with AH can be considered for transplant if they have already failed pharmacotherapy, have strong social and personal supports, are free of psychiatric comorbidities, and are likely to abstain from alcohol [Dureja P, Lucey MR. J Hepatol. 2010]. An algorithm for the diagnosis and management of AH is presented in Figure 3 [Singal S et al. Clin Gastroenterol Hepatol. 2014].
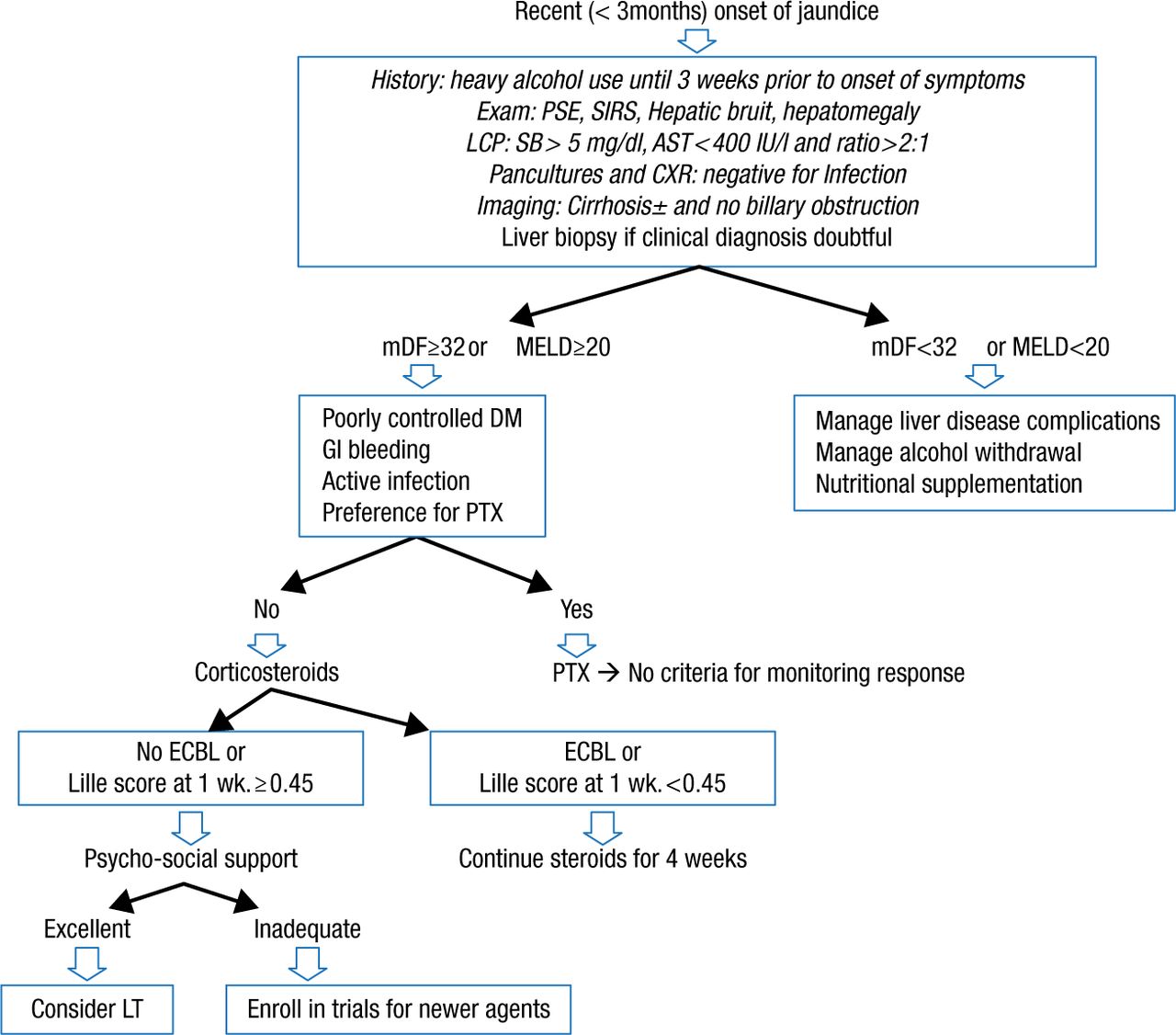
Suggested Algorithm in Diagnosis and Management of Alcoholic Hepatitis
mDF: Modified discriminant function; LCP: Liver chemistry panel; CXR: Chest X-ray; DM: Diabetes mellitus; PTX: Pentoxifylline; ECBL: Early change in bilirubin level; LT: Liver transplantation.
Reprinted from Clin Gastroenterol H, Vol. 12, Singal AK et al, Alcoholic Hepatitis: Current Challenges and Future Directions, Pages No. 555-564, Copyright (2014), with permission from AGA Institute.
In summary, Dr Shah emphasized that ALD will account for an increasing percentage of patients with chronic liver disease. Therefore, there is a need to focus on cost-effective and preventive treatment of these patients and to encourage the development of new and personalized pharmacotherapy approaches.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.