

Summary
In the Micra Transcatheter Pacing Study, a novel leadless pacemaker system delivered using a transcatheter system, was tested for strength duration and battery longevity. Despite its size, the electrical performance of the device was comparable with current ventricular demand pacemakers and utilization of 0.24 vs 0.4 milliseconds pulse width increased the projected battery longevity by 0.83 years.
- leadless transcatheter pacemaker
- battery longevity
- transcatheter pacing system
- Micra TPS
- NCT02004873
- atrial fibrillation
- cardiology & cardiovascular medicine clinical trials
- interventional techniques & devices
Results of the Micra Transcatheter Pacing Study [Ritter P et al. Eur Heart J. 2015], which examined the pacing threshold curve at 3 months following delivery and the projected longevity of a new leadless pacing system delivered using a transcatheter delivery system (TPS), found pacing thresholds were low at the time of implantation and stable at 3 months. Use of a 0.24 vs 0.4 milliseconds pulse width increased the projected battery longevity by 0.83 years noted Clemens Steinwender, MD, Linz University Hospital, Linz, Austria.
The Micra TPS system is a new miniature leadless pacemaker that is interventionally delivered via the femoral vein using a transcatheter delivery system. Because of its small size, the pacing threshold and battery life are of particular interest. Chronaxie is the minimum time (pulse width) required for excitation of a structure (eg, a muscle or nerve) by a voltage of 2 times the rheobase voltage. The rheobase voltage is the threshold at an infinite pulse width. Chronaxie is considered the pulse width that minimizes the use of pacing energy. The Micra TPS device has a nominal pacing pulse width of 0.24 milliseconds, which is close to the chronaxie.
In the Micra Clinical Study, the threshold, impedance, pacing percentage, and heart rate were analyzed in the first 60 patients to reach the 3-month follow-up visit. Pacing threshold measurements were conducted at 0.24, 0.4, and 1.0 milliseconds with a voltage resolution of 0.125 V at implant and 3 months. The Lapicque equation [V = rheobase × (1 + chronaxie / pulse width)] was used to determine chronaxie, rheobase, and the strength duration curve given the 2 measurements at 0.24 and 1.0 milliseconds.
Individual patient battery longevity was projected using programmed pacing amplitude, pulse width, impedance, pacing percentage, and heart rate at the 3-month visit assuming a 5-month shelf life prior to implant.
The most common indication for pacing was atrial fibrillation with pauses. At 3 months, the mean impedance was 651 Ω, mean pacing percentage was 49%, mean heart rate was 72 bpm, and 59 of 60 patients were programmed to a pulse width of 0.24 milliseconds. Impedance decreased and R-waves increased over time.
Mean thresholds at implant were 0.57 at 0.24 milliseconds, 0.46 at 0.4 milliseconds, and 0.37 at 1.0 milliseconds. Mean thresholds at 3 months were 0.51 at 0.24 milliseconds, 0.43 at 0.4 milliseconds, and 0.34 at 1.0 milliseconds. There were 4 and 2 patients with thresholds at 0.24 milliseconds > 1.0 V at implant and 3 months, respectively.
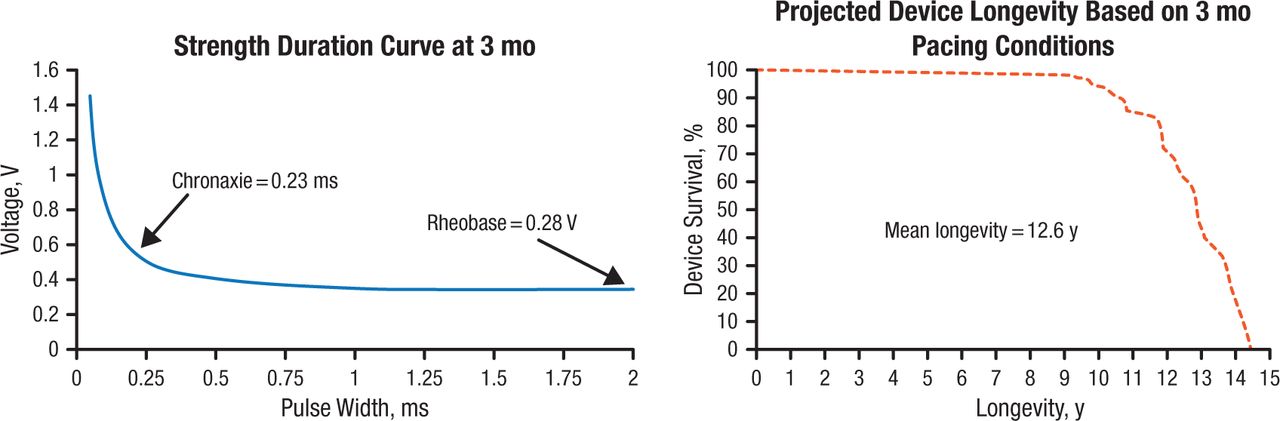
The strength duration curve and projected longevity calculated from 55 patients at 3 months are shown in Figure 1. The mean rheobase was 0.28 V and the chronaxie was 0.23 milliseconds. Battery life was projected at greater than 10 years.
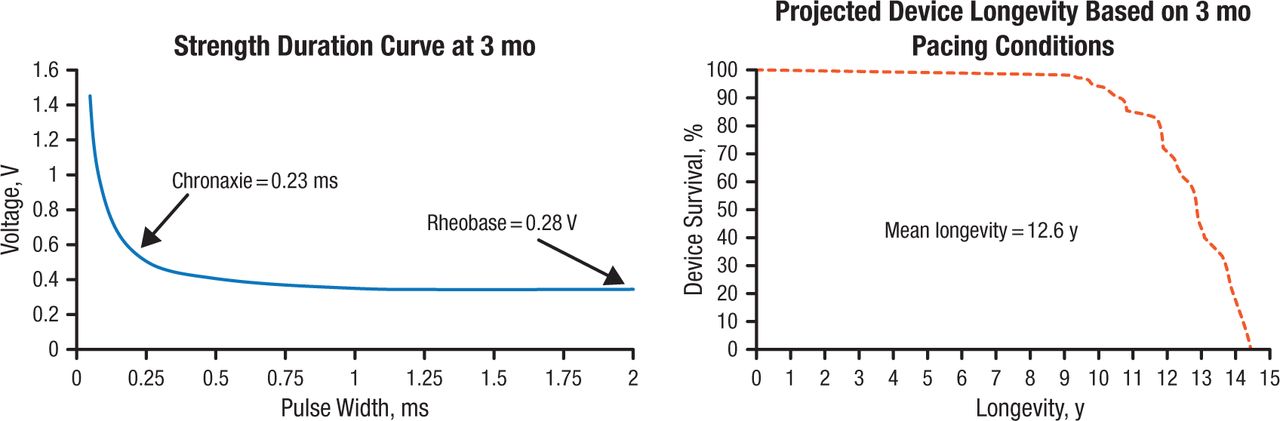
Strength Duration Curve and Projected Device Longevity
Reproduced with permission from C Steinwender, MD.
The findings of this study were limited by the number of patients and relatively short follow-up. In addition, longevity projections assume that pacing threshold, impedance, pacing rate, and pacing percentage do not change after 3 months. However, the estimated longevity of the device is comparable with current ventricular demand pacemakers. The miniature size of this device does not appear to detract from its electrical performance.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.