

Summary
The ADVICE trial substudies show that the rate of pulmonary vein stenosis is low after pulmonary vein isolation with radiofrequency ablation and that the recommendations regarding the duration of the standard blanking period should be revised. The FreezeAF study demonstrates noninferiority of cryoballoon ablation to radiofrequency ablation.
- ADVICE trial
- atrial fibrillation
- blanking period
- cryoballoon ablation
- early recurrence
- FreezeAF trial
- pulmonary vein stenosis
- radiofrequency ablation
- cardiology & cardiovascular medicine clinical trials
- interventional techniques & devices
Atrial fibrillation (AF) is the most commonly encountered clinical arrhythmia, and radiofrequency (RF) catheter ablation involving pulmonary vein isolation (PVI) has emerged as a standard procedure for the treatment of paroxysmal AF. However, this procedure remains technically challenging, with a substantial number of complications that have not been fully examined in large randomized trials.
Sophie Gomes, MD, University of Montreal, Montreal, Quebec, Canada, presented results from a substudy of the ADVICE trial [Macle L et al. Can J Cardiol. 2012], reporting the incidence and characteristics of pulmonary vein (PV) stenosis following catheter ablation of paroxysmal AF, while Boris A. Hoffmann, MD, University Hospital Hamburg-Eppendorf, Hamburg, Germany, presented results of another ADVICE trial substudy, reporting the incidence and significance of early recurrence of atrial tachyarrhythmias (ATs) after catheter ablation for paroxysmal AF. Also, Armin Luik, MD, Karlsruhe Municipal Hospital, Baden-Württemberg, Germany, presented results of the FreezeAF trial [Luik A. Am Heart J. 2010], demonstrating that PVI with a cryoballoon (CB) is as effective as open irrigated RF PVI in patients with paroxysmal AF.
The data on incidence of PV stenosis associated with RF catheter ablation is limited to surveys and small trials, and the methods for determining PV stenosis assessment are not well defined. The analysis presented by Dr Gomes prospectively assessed the incidence and predictors of PV stenosis after RF catheter ablation of AF in the context of the large randomized multicenter ADVICE trial, which evaluated whether adenosine given during the initial PVI procedure may reveal dormant PV conduction, helping to identify the need for additional ablation and leading to improved outcomes.
In the substudy, systematic imaging of the left atrium and PVs was performed at baseline and at 90 days postablation. PV stenosis was defined by a focal narrowing of PV diameter from the maximum adjacent diameter. Stenosis was classified as mild (< 50% narrowing), moderate (50%-70%), and severe (> 70%).
A total of 197 patients were included in this substudy (mean age, 58.9 years; 71% men). PV imaging was performed at a mean of 103 days after PVI. Magnetic resonance imaging was used to assess 65.5% of patients, and a computed tomography scan was used in 34.5%. Severe PV stenosis was not detected in any patients. Moderate stenosis was observed in 5 patients (2.6%), and mild stenosis was identified in 42 patients (21.3%). None of the patients were symptomatic or required any intervention.
Predictive factors of PV stenosis determined in a multivariate analysis were left ventricular ejection fraction (OR, 0.93; 95% CI, 0.88 to 0.99; P = .0144) and diabetes mellitus (OR, 4.30; 95% CI, 1.22 to 15.12; P = .0229).
A significant correlation was observed between assessing PV stenosis using the percentage of reduction in PV diameter and the percentage of reduction in PV area.
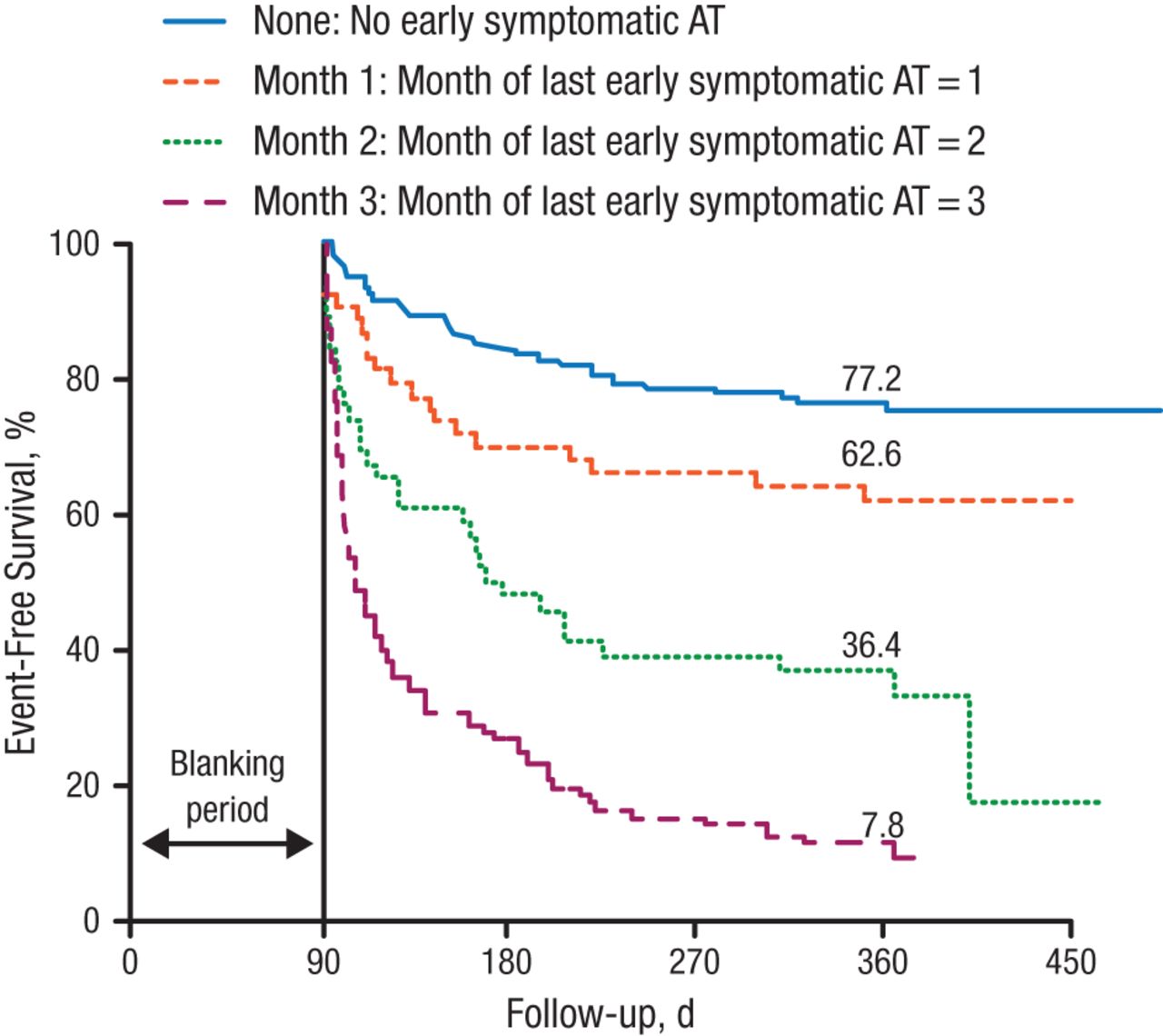
The aim of the substudy presented by Prof Hoffmann was to investigate the clinical outcome in relation to prevalence and timing of early recurrence in the ADVICE trial. A “blanking period” of 3 months after ablation is generally supported by the current guidelines, although the clinical relevance of early recurrence is still debated. The primary end point of the substudy was therefore early recurrence, defined as symptomatic, documented AT ≥ 30 seconds within the first 3 months after ablation.
A total of 179 patients experienced early recurrence. These patients had significantly lower freedom from late recurrence than those with no early recurrence (30.7% vs 77.2%, respectively; P < .0001). Early recurrence persistence >2 months was associated with low long-term freedom from AF when compared with ER exclusively during the first month or the first 2 months (Figure 1). All comparisons were statistically significant (P < .0001).

Freedom From Symptomatic AT After a Single Ablation Procedure
AT, atrial tachyarrhythmia.
Reproduced with permission from BA Hoffmann, MD.
A receiver operating characteristic analysis demonstrated that a blanking period of 50 days would be best for determining long-term success rates following ablation for paroxysmal AF (sensitivity, 0.75; specificity, 0.83; accuracy, 0.78), suggesting that the current recommendations regarding the duration of the blanking period should be revised.
The FreezeAF trial, presented by Dr Luik, was a prospective randomized controlled noninferiority study with a combined primary end point defined as absence of AT > 30 seconds (after the standard 3-month blanking period) and absence of persistent complications at 6 and 12 months after the procedure. Secondary end points included periprocedural complications, total procedure duration, and total x-ray exposure. The main inclusion criteria were age of 18 to 75 years, 2 episodes of paroxysmal AF within the previous 3 months (≥ 1 documented), and documented inefficacy of ≥ 1 antiarrhythmic drugs including a β-blocker.
A total of 291 patients (CB group, 144; RF group, 147) completed the study. All baseline characteristics were well matched between the groups. Freedom from AF without persistent complications was achieved in 65% of patients in the CB group vs 64% in the RF group after a single PVI at 6 months (PNoninferiority = .005) and in 74% in the CB group vs 72% in the RF group after multiple PVI procedures at 12 months (PNoninferiority < .001), as demonstrated by the per-protocol analysis. The intention-to-treat analysis produced similar results.
The mean total procedure time was significantly longer for the RF group compared with the CB group, at 189.1 vs 167.4 minutes, respectively (P = .006). However, the total x-ray dose was significantly higher for CB patients (P = .012), as higher x-ray doses were needed to demonstrate balloon occlusions in this procedure.
The rate of complications was significantly higher in the CB group at 12.2% vs 5.0% in the RF group (P = .021). The difference mainly resulted from a significantly higher rate of phrenic nerve palsy in the CB group compared with the RF group (5.8% vs 0%, respectively; P = .002).
Dr Luik concluded that PVI with CB is noninferior to open irrigated RF PVI in patients with paroxysmal AF.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.