

Summary
Among the controvertible aspects in the use of implantable cardioverter defibrillators to terminate arrhythmias are the risks of inappropriate and appropriate shocks, the apparent enhanced risks of dual-coil over single-coil lead designs, and arguments for and against defibrillator threshold testing at the time of implantation.
- implantable cardioverter defibrillators
- defibrillator threshold testing
- ventricular fibrillation
- antitachycardia pacing
- tachyarrhythmia
- heart failure
- arrhythmias
- interventional techniques & devices
Among the controversies surrounding the use of implantable cardioverter defibrillators (ICDs) for the termination of arrhythmias are the effects of appropriate and inappropriate ICD shocks, the clinical impact of single-coil vs dual-coil leads, and the appropriateness of defibrillator threshold (DFT) testing at the time of ICD implantation.
David T. Huang, MD, University of Rochester Medical Center, Rochester, New York, USA, spoke about the use of antitachycardia pacing (ATP) as applied to ICDs, noting that caregivers must be acutely aware of the appropriate and inappropriate therapies rendered by pacing devices.
The incidence of shock in patients with ICDs remains in excess of 30%, with the rate of appropriate shocks in the range of 17% [Van Rees JB et al. J Am Coll Cardiol. 2011; Daubert JP et al. J Am Coll Cardiol. 2008]. There is a high degree of risk with inappropriate therapy; the risk of mortality is doubled with inappropriate ICD shock, and there is potential for myocardial cell injury, progressive heart failure, and ventricular arrhythmias.
Most clinical trials show at least 60% efficacy of ATP in terminating ventricular tachycardia [Schwab JO. Europace. 2012]. Because of these trials, aggressive use of ATP has been encouraged. The MADIT-RIT trial [Moss AJ et al. N Engl J Med. 2012] found that programming of ICD therapies for tachyarrhythmias ≥ 200 bpm or with a prolonged delay in therapy at ≥ 170 bpm, compared with conventional programming, was associated with a 79% reduction in first occurrence of inappropriate therapy and a 55% reduction in all-cause mortality. The data suggest that inappropriate shocks may not be as benign as previously believed, said Dr Huang, and has prompted a reconsideration of what constitutes optimal programming.
In MADIT-RIT, inappropriate shock (HR, 2.88; 95% CI, 1.02 to 8.17), inappropriate ATP therapy (HR, 3.25; 95% CI, 1.33 to 7.94), and conventional ICD programming (HR, 6.32; 95% CI, 3.13 to 12.75) were independently associated with increased rate of mortality, whereas there was no increase in mortality (HR, 1.02; 95% CI, 0.36 to 2.88) with appropriate ATP only [Ruwald AC et al. Circ Arrhythm Electrophysiol. 2014]. The increased risk of mortality observed in patients receiving appropriate ICD shocks in MADIT-RIT suggests that compromised myocardium may be a contributing factor [Sood N et al. Eur Heart J. 2014].
Monitoring patients (not rendering ATP therapy quickly) who have supraventricular tachycardias with relatively slow heart rates appears to be safe, as found in an unpublished study of a subgroup of 264 MADIT-RIT patients who developed supraventricular tachycardias at a heart rate of 170 to 199 bpm [Zareba W et al. HRS 2014].
Charles J. Love, MD, New York University Langone Medical Center, New York, New York, USA, spoke on the effects of DFTs and lead extraction complications with single- vs dual-coil defibrillator leads. From a review of the literature, he made a case for single-coil leads.
In MADIT-CRT, dual-coil ICD leads were associated with a 1.8 J-lower DFT compared with single-coil leads with a similar first-shock efficacy [Kutyifa J et al. J Cardiovasc Electrophysiol. 2013]. With a mean follow-up of 3.3 years, the risks of atrial tachyarrhythmias, all-cause mortality, and short- and long-term complications including those related to the procedure or the ICD leads were not significantly different. The authors concluded that implantation of single-coil ICD leads may therefore be favorable in most patients.
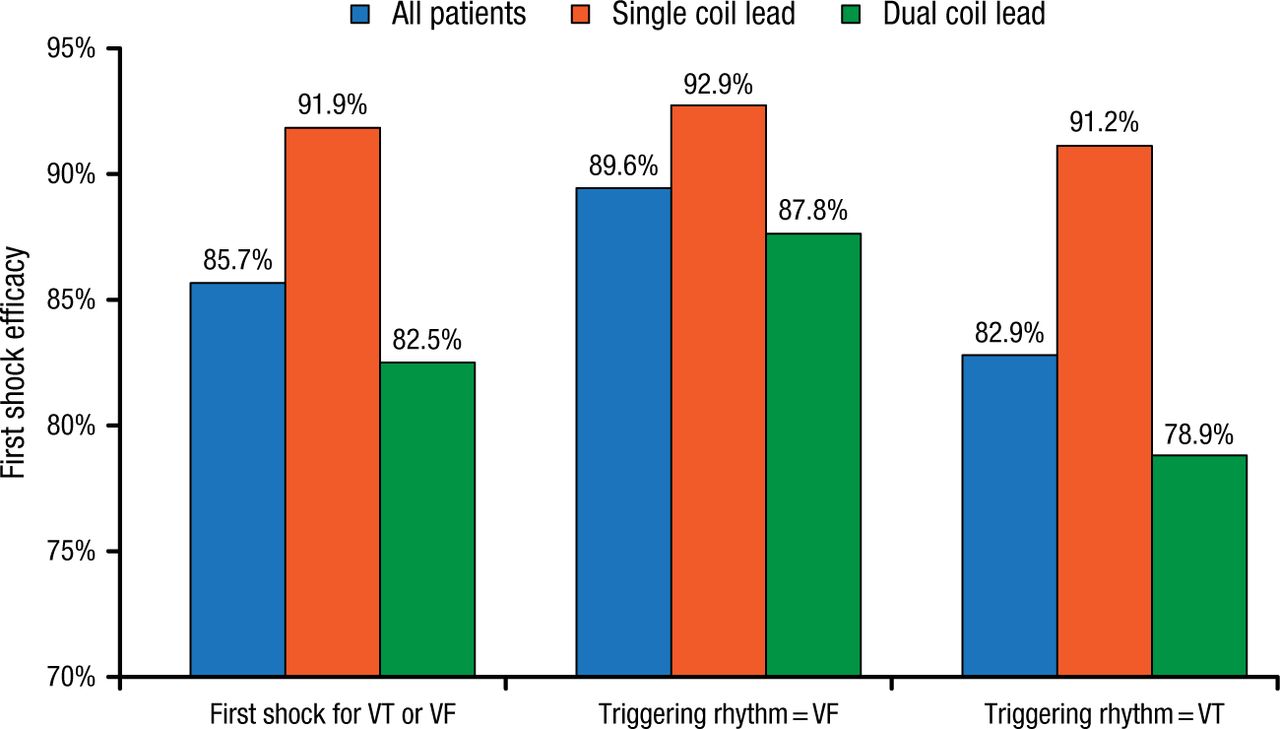
In SCD-HeFT [Aoukar PS et al. Heart Rhythm. 2013], patients with heart failure received a single-lead transvenous ICD, with selection of a dual- vs single-coil right ventricular lead at the physician’s discretion. At 45.5 months of follow-up, there were no significant differences in mortality, sudden cardiac death, first-shock efficacy (Figure 1), and mean DFT between the groups, prompting the authors to advocate a return to single-coil right ventricular ICD leads as the standard of care.

First Shock Efficacy: Single Coil vs Dual Coil
Reprinted from Heart Rhythm, Vol. 10, Aoukar PS et al, No benefit of a dual coil over a single coil ICD lead: Evidence from the Sudden Cardiac Death in Heart Failure Trial, Pages No. 970-976, Copyright (2013), with permission from Elsevier.
The MODALITY study [Baccillieri MS et al. J Interv Card Electrophysiol. 2015] found high rates of successful ICD implantation for both single- and dual-coil transvenous ICD lead systems and no significant difference in interruption of ventricular arrhythmias.
ICD defibrillator coils enable fibrous tissue ingrowth, causing dense vascular and myocardial adhesions, said Dr Love. In studies of ICD lead extraction, dual-coil lead design was an independent predictor of fibrous lead adherence [Segreti L et al. Heart Rhythm. 2014] and all-cause 30-day mortality [Brunner MP et al. Heart Rhythm. 2014]. Dual-coil lead extraction was also found to be riskier in a retrospective analysis of ICD lead extraction at 9 high-volume centers [Epstein LM et al. J Am Coll Cardiol. 2013].
Andrea M. Russo, MD, Cooper University Hospital, Camden, New Jersey, USA, examined the value of routine DFT testing at ICD implantation. In the absence of contraindications, routine DFT testing was previously considered standard of care.
DFT is defined as the minimum shock strength that defibrillates and restores normal rhythm. A safety margin of 10 J below the maximum device output was established in 1988 for termination of ventricular fibrillation (VF). With improvements in device technology, however, an inadequate safety margin for defibrillation at the time of ICD implantation now occurs infrequently, said Dr Russo.
DFT testing is performed at ICD implant to assess electrical integrity of connections between leads and pulse generators, but integrity of connections can be confirmed with delivery of low-voltage pulses. DFT testing is also undertaken to assure reliable sensing and detection of VF, although undersensing of spontaneous VF is extremely rare with modern ICDs, and necessarily not reproducible in an electrophysiology laboratory. Another reason for testing is to ensure successful defibrillation should VF occur after the patient is discharged. But intraoperative DFT testing appears to have little or no beneficial effect on the rates of subsequent successful appropriate shock therapy or arrhythmic death in patients with ICDs, she said. In support of testing, the efficacy of ICDs in clinical trials has been demonstrated using DFT testing, and no large prospective randomized trials have shown similar outcomes without DFT testing.
DFT testing can result in significant complications, including mortality, although this is now relatively uncommon. The increased cost that DFT testing incurs is a potential reason not to do it routinely. However, initial testing remains a reasonable part of ICD placement in some patients, contends Dr Russo. In an unselected series of 1139 patients who underwent initial ICD placement, an inadequate safety margin occurred in about 6%. The percentage of patients who were inappropriate for testing was only 5%.
There are subgroups of patients who may benefit from DFT testing, she concluded, and gaps in evidence exist related to routine omission of testing in some patients, such as those with right-side implants, lead advisories, and totally subcutaneous ICDs. Testing should be individualized in these patients, weighing risks and benefits.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.