

Summary
Patients with atrial fibrillation are at increased risk of stroke, and the addition of a single risk factor indicates a need for prophylaxis with warfarin or a non-VKA oral anticoagulant. Left atrial appendage occlusion is a potential alternative if long-term anticoagulation is contraindicated.
- atrial fibrillation
- AF
- anticoagulation
- OAC
- warfarin
- NOAC
- LAA occlusion
- left atrial appendage
- non-VKA oral anticoagulant
- cardiology & cardiovascular medicine clinical trials
- interventional techniques & devices
Patients with atrial fibrillation (AF) are at an increased risk of stroke, particularly if they have additional risk factors. Therefore, it is important to identify which patients would benefit from oral anticoagulation (OAC) or other treatments such as left atrial appendage (LAA) occlusion according to appropriate risk stratification. Gregory Y.H. Lip, MD, University of Birmingham, Birmingham, United Kingdom, described the role of risk stratification in patients with AF.
Risk factors beyond AF, such as female sex and vascular disease, further increase the risk of stroke [Friberg L et al. Eur Heart J. 2012], which resulted in the development of the CHA2DS2-VASc score [Lip GYH et al. Chest. 2010]. In 2014, the American Heart Association/American College of Cardiology/Heart Rhythm Society guideline for the management of patients with AF changed the recommendation of assessing stroke risk by CHADS2 to CHA2DS2-VASc [January CT et al. Circulation. 2014]. Patients with a CHA2DS2-VASc score ≥ 2 are recommended to receive OAC therapy, with consideration of patient preferences.
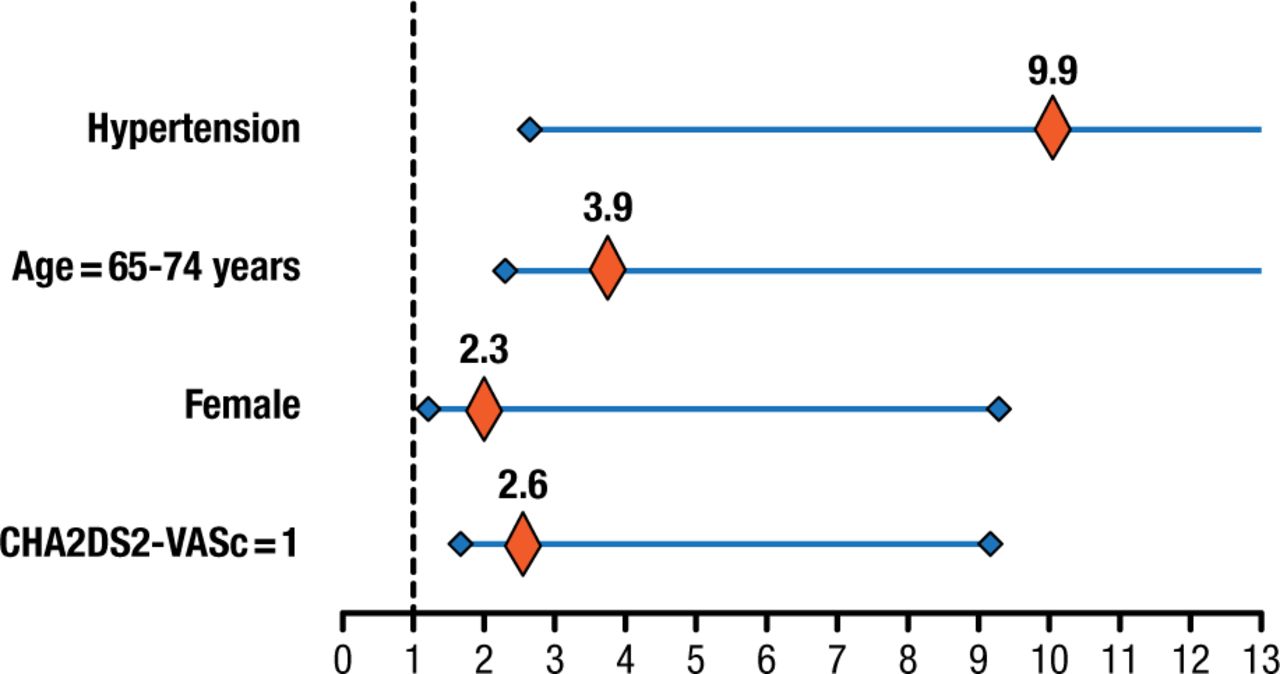
The shift to the CHA2DS2-VASc score was a result of the improvement in risk stratification for patients with a CHADS2 score of 0 to 1 [Olesen JB et al. Thromb Haemost. 2012]. For example, patients with a CHADS2 score of 0 (stroke rate, 1.59; 95% CI, 1.41 to 1.79) were more likely to experience stroke compared with patients with a CHA2DS2-VASc score of 0 (stroke rate, 0.84; 95% CI, 0.65 to 1.08). In an analysis, some components of the CHA2DS2-VASc were found to have a greater effect on risk in patients with a score of 1 (Figure 1) [Huang D et al. Pacing Clin Electrophysiol. 2014]. Similar results were found in another study, suggesting that all patients who have 1 additional risk factor for AF should be considered for OAC [Chao TF et al. J Am Coll Cardiol. 2015].

Varying Degree of Risk Attributed to Individual Components of CHA2DS2-VASc
Relative effects of individual components constituting CHA2DS2-VASc score of 1 on ischemic stroke. Horizontal lines represent 95% confident intervals (CIs) around point estimates.
Reprinted from Huang D et al. Refinement of Ischemic Stroke Risk in Patients with Atrial Fibrillation and CHA2DS2-VASc Score of 1. Pacing Clin Electrophys. 2014; 37: 1442-1447. Copyright © 1999-2015 John Wiley & Sons, Inc.
Once it is determined that a patient has AF and would benefit from OAC, physicians must choose whether to initiate a vitamin K antagonist (VKA), such as warfarin, or a non-VKA oral anticoagulant (NOAC). A. John Camm, MD, St. George’s University of London and Imperial College, London, United Kingdom, discussed the reduction of stroke risk in AF by OACs.
The efficacy of VKAs has been established in reduction of stroke in patients with AF [Hart RG et al. Ann Intern Med. 2007]. Yet there are problems with warfarin use, such as maintaining a high time in therapeutic range (TTR), as low TTR is associated with an increased risk of stroke [Morgan CL et al. Thromb Res. 2009]. However, Prof Camm pointed out that warfarin remains the standard of care in certain cases: for patients with a mechanical heart valve, severe renal impairment, or intolerance to NOACs; if cost is an issue; and if there is a risk of noncompliance.
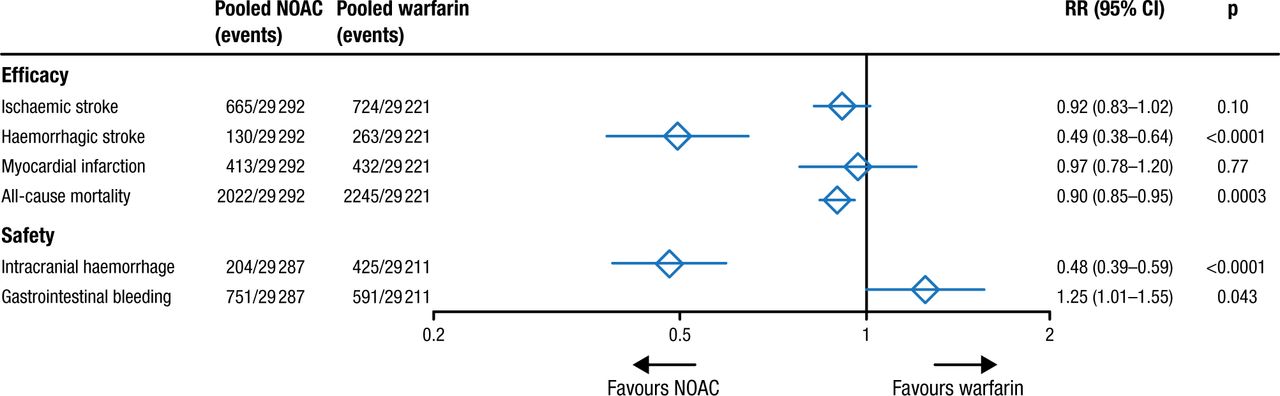
In a meta-analysis of the 4 pivotal trials of the NOACs (RE-LY, ROCKET AF, ARISTOTLE, and ENGAGE AF-TIMI), which included data from > 71 000 patients with AF, dabigatran and apixaban were favored for reduction of stroke and systemic embolism, whereas apixaban and edoxaban were favored for a lower risk of major bleeding compared with warfarin [Ruff CT et al. Lancet. 2013]. A major advantage of the NOACs over warfarin is the reduced risk of hemorrhagic stroke and intracranial hemorrhage (Figure 2).

Meta-analysis of the NOAC Pivotal Trials
Data are n/N, unless otherwise indicated. Heterogeneity: ischaemic stroke I2=32%, p=0.22; haemorrhagic stroke I2=34%, p=0.21; myocardial infarction I2=48%, p=0.13; all-cause mortality I2=0%, p=0.81; intracranial haemorrhage I2=32%, p=0.22; gastrointestinal bleeding I2=74%, p=0.009. NOAC=new oral anticoagulant. RR=risk ratio.
Reprinted from The Lancet, Vol. 383, Ruff CT et al, Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials, Pages No. 955-962, Copyright (2014), with permission from Elsevier.
Despite the advantages of the NOACs, there are concerns regarding a lack of monitoring, the inability to measure the degree of anticoagulation, the effect of nonadherence due to the short half-lives, lack of an antidote and questions of how to manage major bleeding, and the expense of the agents. In addition, renal impairment can be an issue in particular with dabigatran because it has a high rate of renal clearance. Although the NOACs have fixed dosing with no need for regular monitoring, questions have arisen about the association between plasma concentration of dabigatran and the risk of stroke and bleeding. The RE-LY trial indicated that, after considering patient characteristics such as previous stroke and age, tailoring the dose of dabigatran to achieve an appropriate plasma concentration would be difficult and is unlikely to reduce the risk of bleeding [Reilly PA et al. J Am Coll Cardiol. 2014].
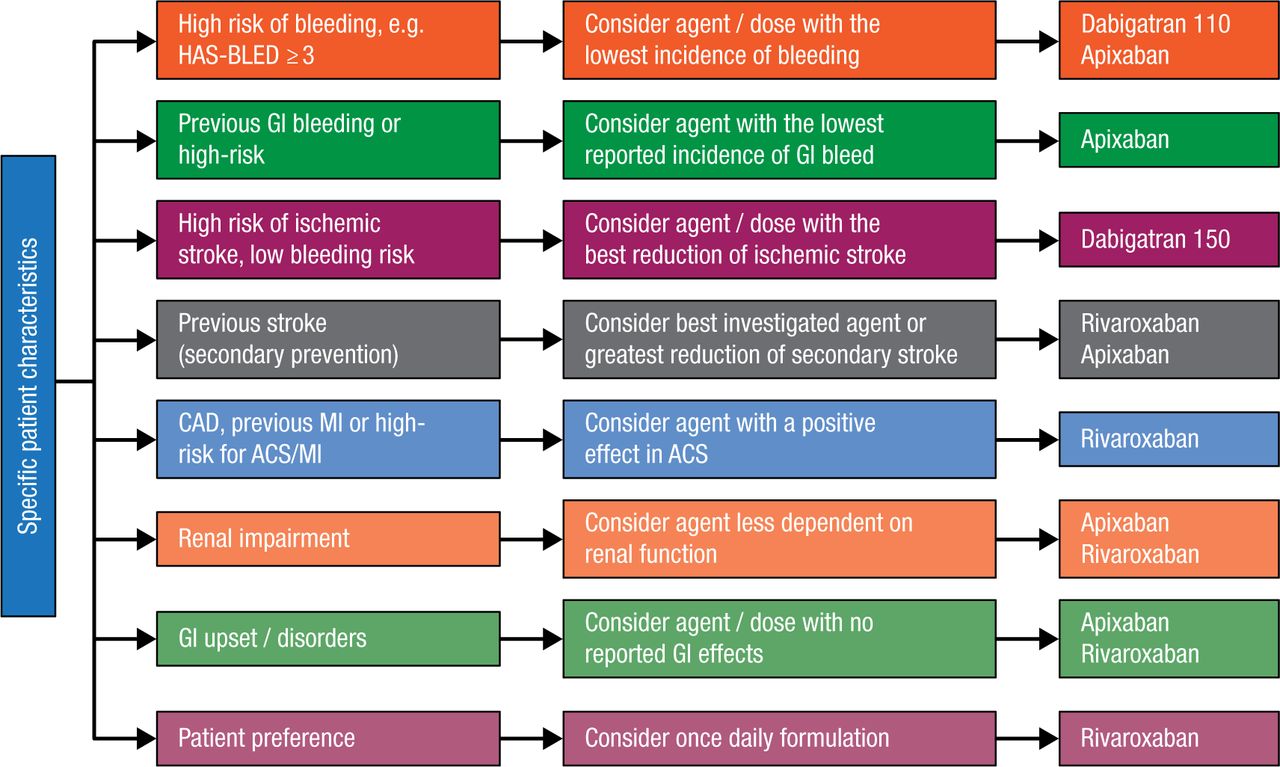
Prof Camm acknowledged that determining which OAC to use was challenging, as there are no head-to-head trials among the NOACs; therefore, data from multiple sources and patient characteristics should be considered. He presented an algorithm that could be helpful when determining which NOAC to prescribe; however, he emphasized that all of the points are debatable (Figure 3) [Savelieva I, Camm AJ. Clin Cardiol. 2014].

Guidance for Determining Which NOAC to Prescribe
Possible considerations (authors’ opinions) for selecting between novel oral anticoagulants (if preferred to a vitamin K antagonist) based on patient characteristics in the absence of head-to-head trials. Any clinical decision should take account of individual patient presentation and agent/dose availability based on local regulatory approval. Clinical opinions are often based on indirect comparisons, subgroup analyses, adverse event profiles, and clinical trials in other patient populations. None of these data on which a choice will be made is individually valid, and together only provide a gestalt, but in the absence of other information clinicians have no other way to proceed. Abbreviations: ACS, acute coronary syndrome; AF, atrial fibrillation; CAD, coronary artery disease; GI, gastrointestinal; HAS-BLED, hypertension, abnormal renal/liver function (1 point each), stroke, bleeding history or predisposition, labile international normalized ratio, elderly (≥65 years), drugs/alcohol concomitantly (1 point each); MI, myocardial infarction.
Reprinted from Savelieva I et al. Practical Considerations for Using Novel Oral Anticoagulants in Patients With Atrial Fibrillation. Clin Cardiol. 2013; 37: 32-47. Copyright 2013 Wiley Periodicals, Inc.
An alternative to OAC for the reduction of stroke risk in AF may be LAA occlusion via surgical amputation and closure, or with percutaneous devices. Richard Whitlock, MD, PhD, McMaster University, Hamilton, Ontario, Canada, described LAA occlusion in patients with AF. The LAA is a remnant of the embryonic left atrium and functions as a reservoir for atrial natriuretic peptide; however, its hemodynamic role is not well understood.
About 70% of strokes that occur in patients with AF originate in the LAA. Prof Whitlock proposed that if the LAA is an unnecessary structure and it is implicated in the majority of strokes in patients with AF, then its removal may be an ideal option. The multicenter, randomized LAAOS III trial is currently underway, in which LAA occlusion will be evaluated in patients with AF who are undergoing cardiac surgery [Whitlock R et al. Ann Cardiothorac Surg. 2014].
Rigorous, randomized, controlled trials are needed to further define the role of LAA occlusion in the reduction of stroke and systemic embolism in patients with AF. However, based on the current low quality of data, Prof Whitlock stated that the procedure must be considered as an alternative for patients who have a contraindication to long-term OAC therapy.
In conclusion, the presence of AF is associated with an increased risk of stroke, with the risk rising with higher duration and frequency of the abnormal rhythm. There are now multiple OACs available for the reduction of stroke and systemic embolism in these patients, and in patients who are not candidates for OAC, LAA occlusion may be an alternative.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.