

Summary
The observational CREDO study of Riata silicone endocardial defibrillation leads demonstrates that the average rate of electrical failure for 7 French and 8 French Riata leads was 5.9% over a mean follow-up of 7.5 years, with a trend toward a higher failure rate with cable externalization with 8 Fr leads.
- cable externalization
- CREDO
- electrical failure
- Riata leads
- cardiac implantable electronic devices
- cardiology & cardiovascular medicine clinical trials
Ratika Parkash, MD, Queen Elizabeth II Health Sciences Centre, Halifax, Nova Scotia, Canada, presented results of the Canadian Registry of Cardiac Implantable Electronic Device Outcomes (CREDO) study, demonstrating that over a mean follow-up of 7.5 years, the rate of electrical failure was similar for 7 French (Fr) and 8 Fr Riata leads, with an average failure rate of 5.9%.
Cable externalization and insulation abrasion are known to occur with Riata silicone endocardial defibrillation leads. The electrical and structural failure rates have been described, but the current rates are not known. Also, the relationship of cable externalization to electrical failure is not well described.
CREDO was a prospective, observational cohort study that involved 15 Canadian centers. The overall objective was to perform an observational study of Riata leads under advisory in Canada. The specific objectives were to determine the electrical and structural failure rates of the leads over time and to determine the predictors of such failure.
The patient population included patients with a St Jude Medical Riata model implanted under advisory in Canada. Patients were followed as per Canadian guidelines for device follow-up. Radiographic screening was not mandated and was left up to the discretion of each center. The end points were death attributable to lead malfunction, incidence of cable externalization, and incidence of electric lead failure.
A total of 2707 patients were observed (mean age 63.2 years; 19.3% women) with a mean follow-up time of 7.47 years. Across all centers, 8 Fr leads were used in 70.2% of cases and 7 Fr leads were used in 29.8% of cases.
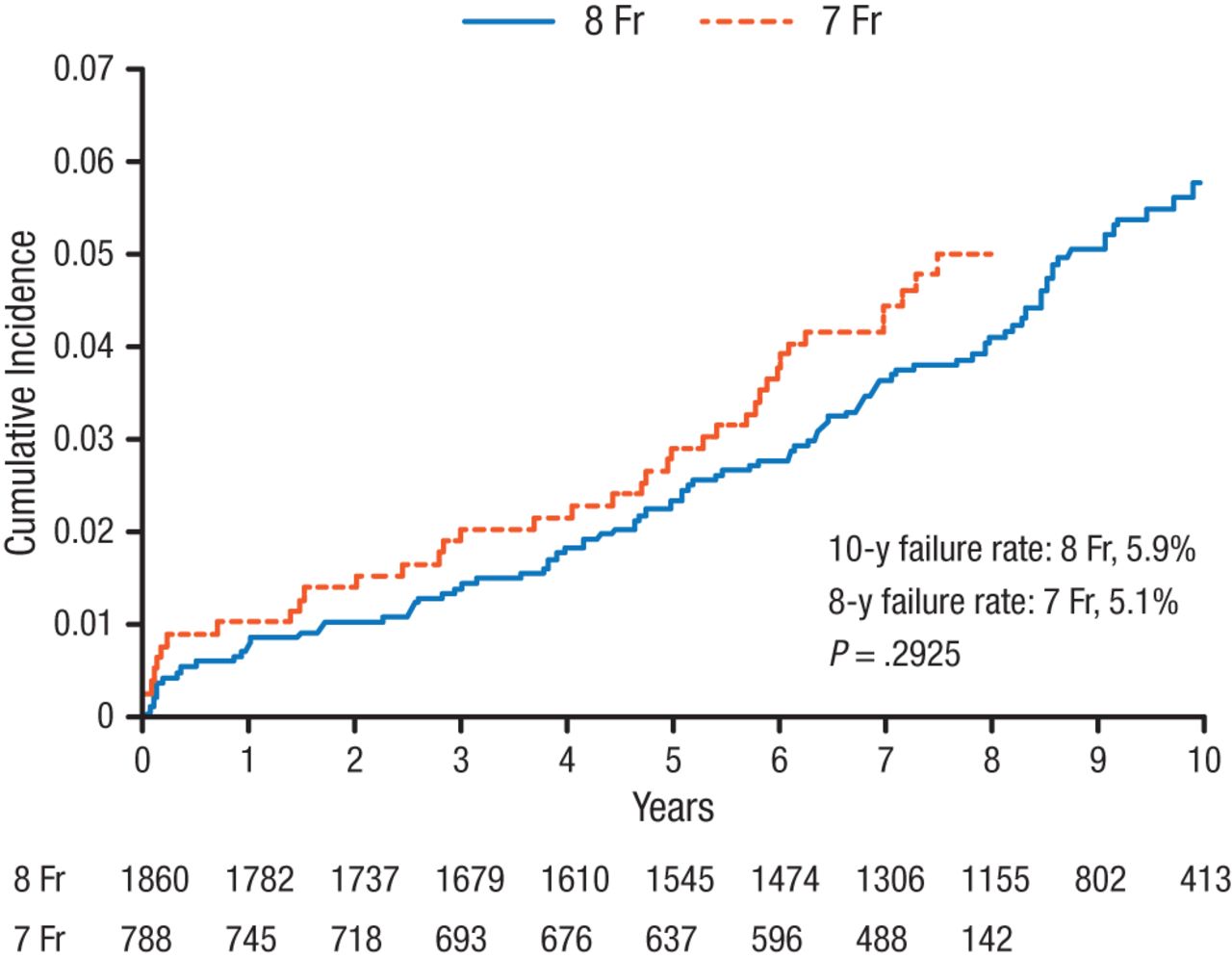
On average, 8 Fr leads had a longer follow-up and the 10-year failure rate of 8 Fr leads was 5.9%, while an 8-year failure rate of 7 Fr leads was 5.1% (Figure 1). The difference was not statistically significant, and the average failure rate was 5.9% over a mean follow-up of 7.5 years.

Cumulative Incidence of Electrical Failure
Fr, French.
Reproduced with permission from R Parkash, MD.
Cable externalization occurred at a rate of 7.4% in 8 Fr leads vs 4.9% in 7 Fr leads, mainly occurring after 4 years of follow-up. Among patients who underwent radiographic screening (n = 1187), cable externalization occurred in 6.7% of all patients. A total of 10.1% of patients experienced cable externalization with electrical failure (9.4% with 8 Fr leads vs 13.3% with 7 Fr leads).
Multivariate predictors of lead failure were younger age (HR, 0.84; 95% CI, 0.75 to 0.95; P < .01; per 10 years) and higher left ventricular ejection fraction grouped into 10% deciles (HR, 1.26; 95% CI, 1.10 to 1.45; P < .01).
The risk of major complications in lead revisions was 6.32%. Complications included infection, pneumothorax, death, lead dislodgement, reoperation, and hematoma.
Dr Parkash concluded that over a mean follow-up of 7.5 years, the rate of electrical failure was similar for 7 Fr and 8 Fr Riata leads. There was a trend toward a higher failure rate with cable externalization with 8 Fr leads. The risk of major complications in lead revisions at 6.3% was similar to the rate of electrical failure (5.9%). Finally, Dr Parkash stressed that isolated lead revision or extraction due to advisory is not warranted.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.