

Summary
The primary reason for hospitalization among patients with acute heart failure (AHF) is congestion, for which the most common treatment is intravenous loop diuretics [Mentz RJ et al. Eur J Heart Fail 2014]. However, many patients fail to respond or have an inadequate response to this treatment and are discharged without weight loss and with continued signs of congestion. This article discusses the results of a sub-analysis of data from the Relaxin for the Treatment of Acute Heart Failure trial [RELAX-AHF; Teerlink JR et al. Lancet 2013].
- Cardiology Clinical Trials
- Heart Failure
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Heart Failure
The primary reason for hospitalization among patients with acute heart failure (AHF) is congestion, for which the most common treatment is intravenous loop diuretics [Mentz RJ et al. Eur J Heart Fail 2014]. However, many patients fail to respond or have an inadequate response to this treatment and are discharged without weight loss and with continued signs of congestion. Adriaan Voors, MD, PhD, University Medical Center, Groningen, the Netherlands, presented the results of a sub-analysis of data from the Relaxin for the Treatment of Acute Heart Failure trial [RELAX-AHF; Teerlink JR et al. Lancet 2013], which showed that poor diuretic response was independently associated with residence in a Western-like region, lower diastolic blood pressure (DBP), lower levels of aspartate aminotransferase (AST) and potassium, higher blood urea nitrogen (BUN), and an absence of edema. Serelaxin use was associated with lower doses of intravenous loop diuretics and slightly less weight loss, resulting in a neutral effect on diuretic response.
Although the mechanism of diuretic resistance is not entirely understood, it is thought to result from the complex interplay between cardiac and renal dysfunction and specific renal adaptation mechanisms. Serelaxin, a recombinant form of human relaxin-2, is a vasodilator that is also associated with decreased inflammation, fibrosis and pro-angiogenic effects [Teichman SL et al. Curr Heart Fail Rep 2010]. In the RELAX-AHF trial, serelaxin was associated with dyspnea relief as well as a reduction in cardiovascular mortality [Teerlink JR et al. Lancet 2013]. It has also been shown to improve markers of renal function (creatinine, cystatin C, and BUN) [Metra M et al. J Am Col Cardiol 2013].
The objective of the sub-analysis presented by Prof. Voors was to establish the characteristics and clinical outcomes related to diuretic response and to determine the effect of serelaxin on diuretic response among patients hospitalized with AHF. For the RELAX-AHF trial, 1161 subjects were randomly assigned to standard care plus 48-hour intravenous infusions of placebo or serelaxin (30 µg/kg/day) within 16 hours of presentation. All patients had dyspnea, congestion on chest radiographs, increased levels of brain natriuretic peptide (BNP) or N-terminal pro-hormone of BNP, mild-to-moderate renal insufficiency (estimated glomerular filtration rate, 30 to 75 mL/minute), and systolic blood pressure above 125 mm Hg. Diuretic response was defined as weight lost (kg) with 40 mg IV or 90 mg oral furosemide (or equivalent loop diuretic) up to Day 5. Patients were subdivided based on tertiles of diuretic response.
A poor diuretic response was independently associated with residence in a Western-like region, lower DBP, lower levels of AST and potassium, higher BUN, and the absence of edema (Table 1).
Multivariate Predictors of Poor Diuretic Response
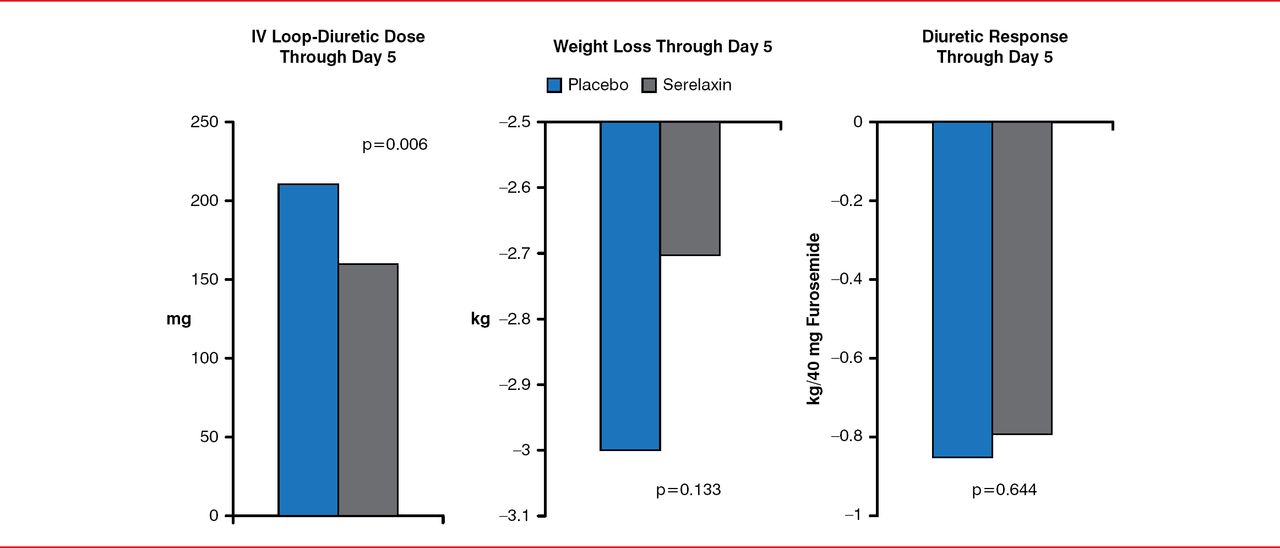
Serelaxin use was associated with lower doses of intravenous loop diuretics and slightly less weight loss, resulting in a neutral effect on diuretic response (Figure 1). Poor diuretic response was independently associated with less relief of dyspnea and significantly higher risk of death or re-admission through Day 60 (p<0.0001).

Serelaxin and Diuretic Response
Reproduced with permission from A Voors, MD, PhD.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.