

Summary
The MILLION study shows that aggressive, simultaneous treatment with an amlodipine- and statin-based regimen lowers blood pressure and low-density lipoprotein cholesterol to a greater extent than standard intensity treatment in a Japanese population. However, percent change in coronary plaque volume, and lumen and vessel volume were similar among both treatment arms.
- statin
- amlodipine
- blood pressure
- plaque
- coronary artery disease
- low-density lipoprotein cholesterol
- LDL-C
- cardiology & cardiovascular medicine clinical trials
An aggressive, simultaneous amlodipine- and statin-based regimen significantly decreased blood pressure (BP) and low-density lipoprotein cholesterol (LDL-C) compared with a standard-intensity regimen in a Japanese population with coronary artery disease (CAD). Masa-aki Kawashiri, MD, Kanazawa University, Kanazawa, Japan, presented these unpublished data from the MILLION study.
Intensive statin therapy for lowering LDL-C had been demonstrated to reduce the risk of major adverse cardiovascular events compared with moderate-intensity statin therapy. In addition, lowering BP with an amlodipine-based regimen also reduced major adverse cardiovascular events in patients with hypertension compared with a β-blocker or angiotensin-converting enzyme inhibitor–based regimen. However, the combination of both LDL-C and BP lowering did not affect outcomes compared with standard therapy [Kohro T et al. Circ J. 2011]. The purpose of the MILLION trial was to evaluate the change in plaque volume using intravascular ultrasonography, BP, and lipids in a Japanese population with CAD.
In the open-label, multicenter MILLION study, 100 patients with CAD who underwent percutaneous coronary intervention were randomly assigned to receive standard therapy with amlodipine 2.5 mg and atorvastatin 5 mg and other agents as necessary to reduce BP to < 140/90 mm Hg and LDL-C to < 100 mg/dL, or aggressive treatment with amlodipine 5 mg and atorvastatin 10 mg and other agents to decrease BP to < 120/70 mm Hg and LDL-C to < 70 mg/dL [Kawashiri MA et al. Heart Vessels. 2014]. Patients were excluded if the percutaneous coronary intervention was unsuccessful, they had type 1 diabetes or poorly controlled diabetes, they were receiving insulin therapy, had secondary hypertension, were using dihydropyridine calcium channel antagonist for > 6 months, used an intensive lipid-lowering statin agent, had familial hypercholesterolemia, or were aged ≥ 80 years. Baseline characteristics were similar between the 2 arms.
Among the 68 patients who completed the study, the primary end point of this study, the percent change in coronary plaque volume, decreased in the standard treatment arm (n = 33; P = .006) and the aggressive treatment arm (n = 35; P = .008), but there were no differences between the 2 therapies. In addition, BP and LDL-C were significantly reduced in both arms, with a greater reduction in the aggressive treatment arm compared with the standard treatment arm (BP, P = .0009; LDL-C, P = .007; Figure 1). There was no significant difference in percent change in lumen and vessel volume between the 2 arms.
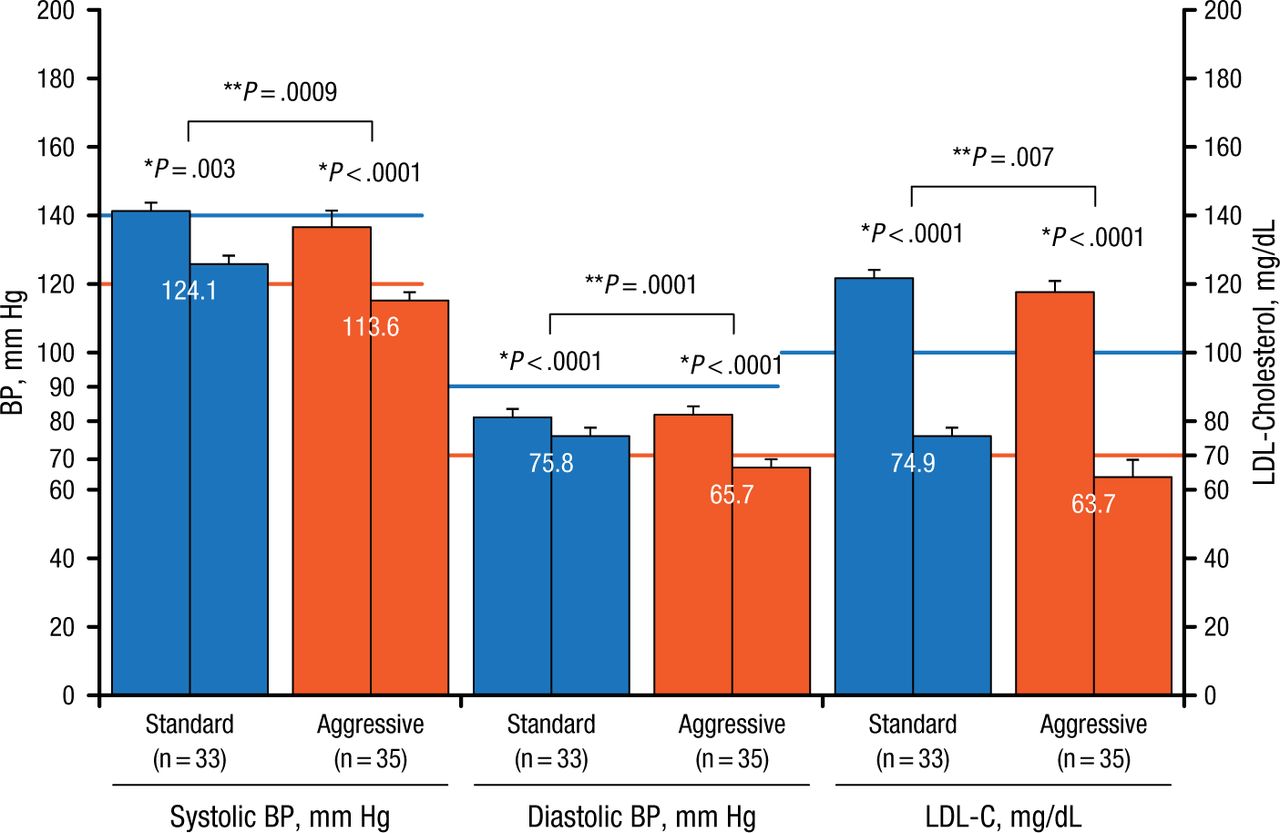
Effect of Aggressive Therapy for BP and LDL-C Lowering
BP, blood pressure; LDL-C, low-density lipoprotein cholesterol.
*Paired t-test.
**Unpaired t-test.
Reproduced with permission from M Kawashiri, MD.
Dr Kawashiri concluded that the data from the MILLION trial suggest that both standard and aggressive BP and lipid-lowering regimens were effective; however, a greater decrease in BP and LDL-C was evident in the aggressive treatment group compared with standard therapy.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.