

Summary
The MR CLEAN trial evaluates the effect of intra-arterial intervention in proximal anterior circulation acute ischemic stroke. Endovascular therapy within 6 hours of onset improves functional outcomes compared with standard guideline stroke treatment. Intervention is beneficial, in particular, to patients older than 80 years and those in the lower modified NIH Stroke Scale categories.
- Intra-arterial intervention
- endovascular therapy
- proximal intracranial arterial occlusion
- acute ischemic stroke
- modified Rankin Scale
- MR CLEAN
- ISRCTN10888758
- neurology clinical trials
- cerebrovascular disease
- interventional techniques & devices
- ischemia
Diederik Dippel, MD, PhD, Erasmus University Medical Center, Rotterdam, the Netherlands, presented updated data from MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke (AIS) in the Netherlands [ISRCTN10888758]. The results demonstrated improved functional outcomes in patients who received endovascular therapy up to 6 hours after stroke onset in the proximal anterior circulation, in addition to best medical care [Berkhemer OA et al. N Engl J Med. 2015].
According to Prof Dippel, more than one-third of patients with AIS have a proximal intracranial arterial occlusion. Intravenous (IV) administration of tissue plasminogen activator (tPA) within 4.5 hours of stroke onset clears the blockage in only about one-third of these and leads to recovery in only 10%.
Although previous trials showed no effect of intra-arterial treatment on functional outcomes in AIS, a new study was needed, he stressed, owing to improved patient selection from widespread use of computed tomography, rapid access to treatment in the Netherlands, and new endovascular treatment modalities. Prof Dippel and colleagues therefore conducted MR CLEAN to evaluate the effect of intra-arterial treatment on functional outcome in AIS, on a background of best medical management.
The open-label trial [Berkhemer OA et al. N Engl J Med. 2015] included 500 patients (≥ 18 years) with AIS with cranial arterial anterior circulation occlusion that was confirmed on imaging and could be treated intra-arterially within 6 hours of symptom onset. NIH Stroke Scale (NIHSS) scores were ≥ 2. The primary outcome was the score on the modified Rankin Scale (mRS) at 90 days.
Participants received usual care (which could include IV alteplase) and were randomized to also receive either intra-arterial intervention (n = 233) or no additional treatment (n = 267). The time from onset to groin puncture in the intervention group was 260 minutes.
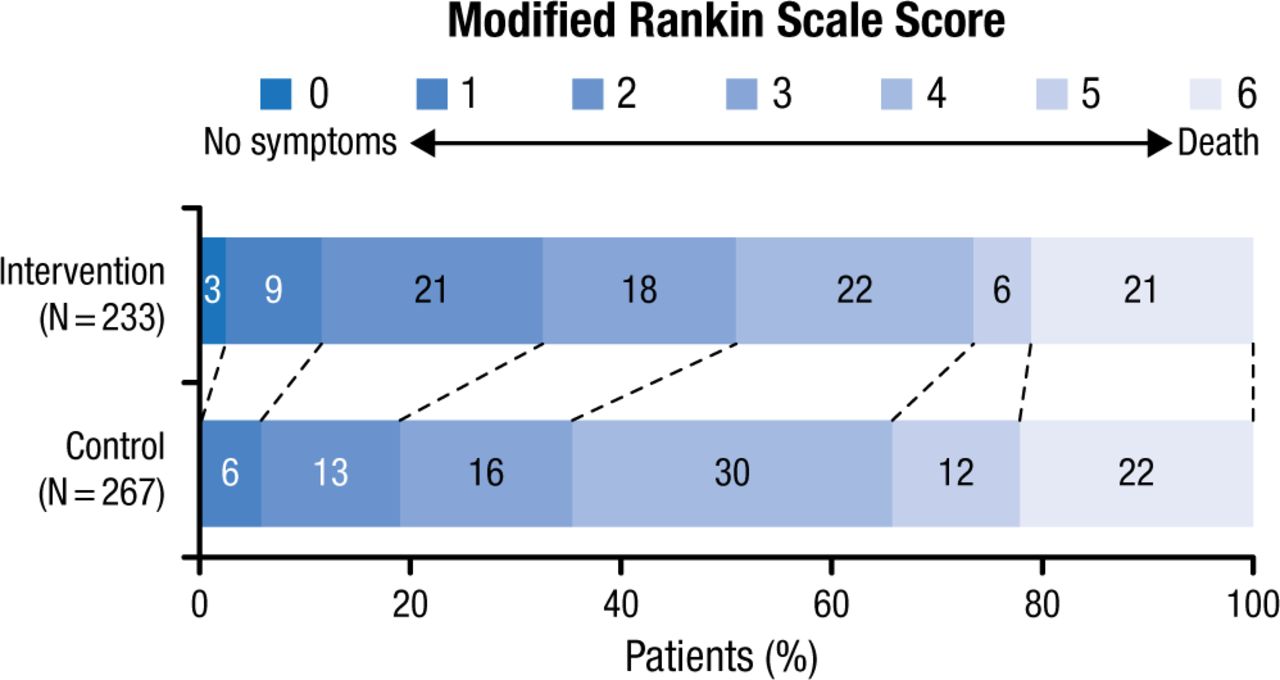
Patients in the intervention group had lower mRS categories, consistent with improved function, at 90 days (adjusted OR, 1.67; 95% CI, 1.21 to 2.30; Figure 1).
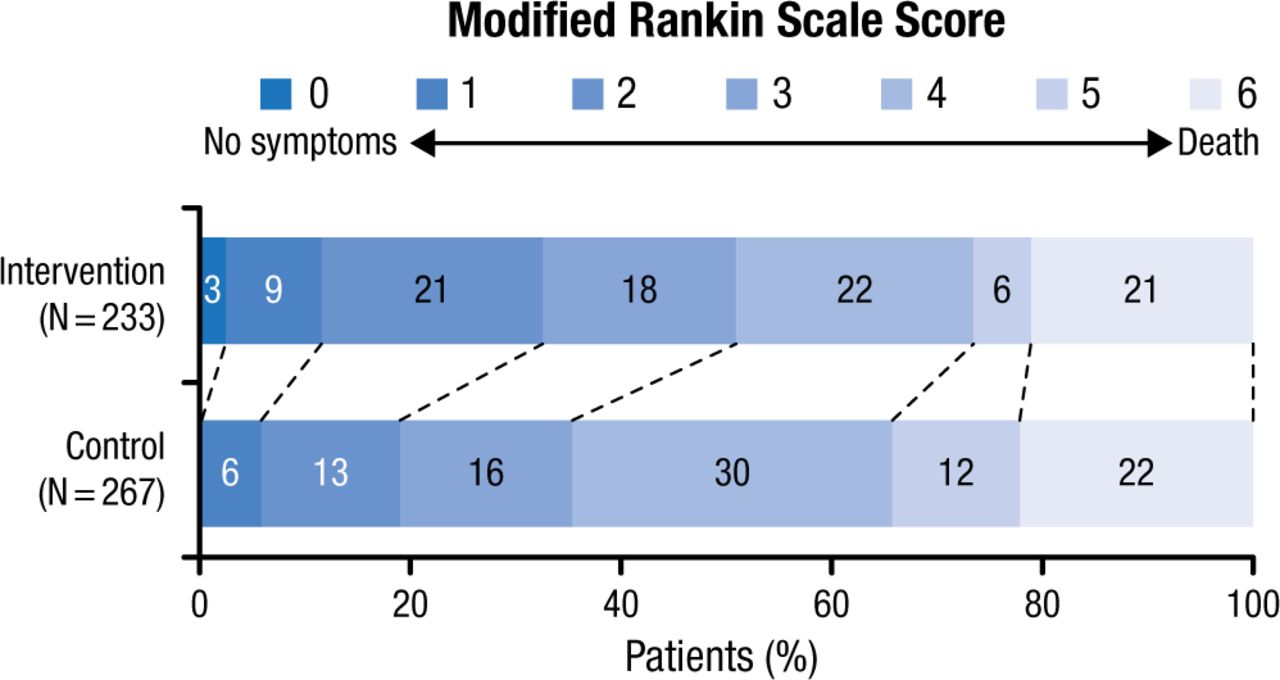
Effect of Endovascular Intervention on Functional Outcome at 90 Days
From N Engl J Med, Berkhemer OA et al., A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke, Volume No. 372, 11-20. Copyright © (2015) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Prof Dippel also highlighted unpublished subanalyses from MR CLEAN. Intra-arterial intervention was superior to no additional treatment for all age groups in the study, in particular, for those aged ≥ 80 years (adjusted OR, 3.24; 95% CI, 1.22 to 8.62), and for those with the most severe strokes (NIHSS score ≥ 20; adjusted OR, 1.85; 95% CI, 1.06 to 2.31).
Compared with controls, intra-arterial intervention with local anesthesia (adjusted OR, 2.79; 95% CI, 1.70 to 4.59) was more likely to result in a good outcome than general anesthesia (adjusted OR, 1.09; 95% CI, 0.56 to 2.12), which showed no benefit over usual care.
Prof Dippel concluded that intra-arterial intervention on a background of usual best stroke care is effective and safe in many patients if provided within 6 hours of stroke onset.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.