

Summary
Sorafenib and lenvatinib can be effective for advanced differentiated thyroid cancer, and vandetanib and cabozantinib can be effective options for advanced medullary thyroid cancer. When first-line tyrosine kinase inhibitors fail for patients, evidence supports salvage therapy for differentiated thyroid cancer but is less compelling for medullary thyroid cancer.
- differentiated thyroid cancer
- medullary thyroid cancer
- sorafenib
- lenvatinib
- vandetanib
- cabozantinib
- thyroid disorders
The systemic therapies sorafenib and lenvatinib, which target the vascular endothelial growth factor (VEGF) pathway, are treatment options for advanced differentiated thyroid cancer (DTC). In advanced medullary thyroid cancer (MTC), vandetanib and cabozantinib are meaningful options. For patients who experience failure of a first-line tyrosine kinase inhibitor (TKI), salvage therapy is a reasonable strategy in DTC but has less evidence to support its use in MTC.
Manisha H. Shah, MD, Ohio State University Comprehensive Cancer Center, Columbus, Ohio, USA, discussed the recently approved targeted therapies for advanced DTC: sorafenib and lenvatinib. She explained that BRAF is a key player in papillary thyroid cancer and that about 70% of patients in the clinical trial population have the BRAF mutation.
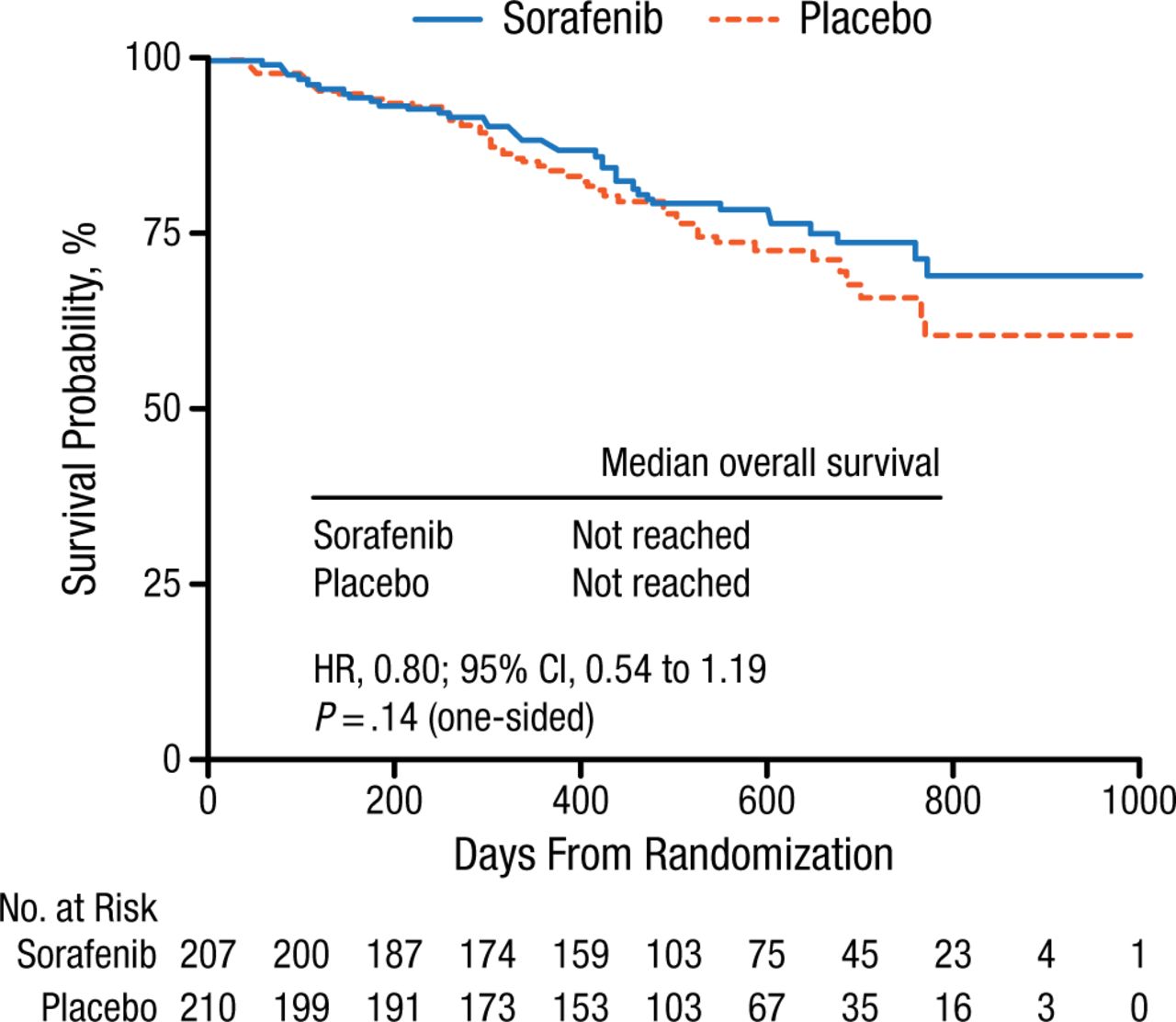
Sorafenib is a BRAF inhibitor that is a multikinase inhibitor (MKI) whose targets include the VEGF receptors. The DECISION trial was a multicenter, international, double-blind, phase 3 trial that enrolled patients with DTC that was locally advanced or metastatic and iodine refractory and randomized them 1:1 to either sorafenib or placebo [Brose MS et al. Lancet. 2014]. The primary end point of median progression-free survival (PFS) was 10.8 months for patients receiving sorafenib (n = 207) and 5.8 months for those receiving placebo (n = 210; HR, 0.59; 95% CI, 0.45 to 0.76; P < .0001; Figure 1). The partial response (PR) rate was only 12%, with a median duration of about 10 months. Adverse events (AEs) led to dose reductions in 66% of patients and discontinuation in 18%. Hypocalcemia of grade 3 or 4 can occur with sorafenib, although it is preventable and quickly treatable. Keratoacanthoma is a notable class effect of BRAF inhibitors.
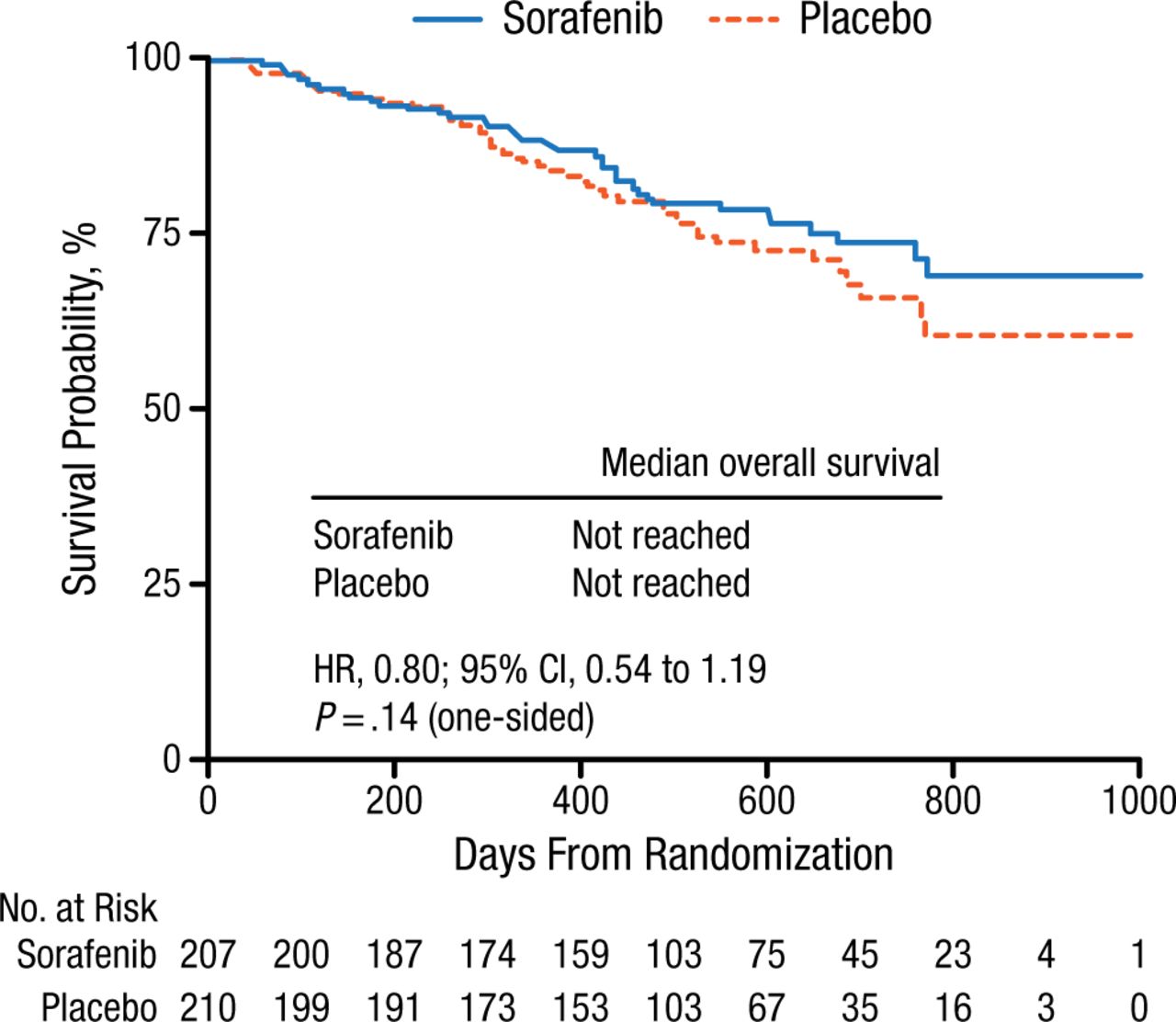
Progression-Free Survival in the DECISION Trial of Sorafenib vs Placebo
Reprinted from Lancet, 384, Brose MS et al, Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomized, double-blind, phase 3 trial, 384:319-328, Copyright (2014), with permission from Elsevier.
Lenvatinib targets particular fibroblast growth factor receptors, which might evoke unique responses. The SELECT study was a phase 3 pivotal trial with a median PFS (the primary end point) of 18.3 months for the patients receiving lenvatinib (n = 261) and 3.6 months for those receiving placebo (n = 131; HR, 0.21; 99% CI, 0.14 to 0.31; P < .001) [Schlumberger M et al. N Engl J Med. 2015]. PRs were achieved by 63% of patients receiving lenvatinib, and complete responses were achieved by 2%. AEs led to dose reductions in 68% of patients and discontinuation in 14% of patients. Response to lenvatinib was not predicted by RAS or BRAF mutations.
Notably, treatment with MKIs with angiogenic targets can lead to the rare but dangerous and potentially fatal AEs of bowel perforation and fistulas, bleeding in the tumor or other organs, thromboembolism, and cardiac effects that can include arrhythmias, coronary artery disease, and LV dysfunction. These affect 1% to 2% of patients.
Ezra E.W. Cohen, MD, University of California San Diego, La Jolla, California, USA, discussed the treatment of MTC, which accounts for about 5% of thyroid cancers. Distant metastases carry a poor prognosis with a median overall survival (OS) of about 2 years. Among MTC, 75% are sporadic and about 65% are RET mutated. Hereditary MTC is almost universally RET mutated.
Patients with metastatic or recurrent disease that is not curable do not necessarily require therapy and may be better served by observation. Ideally, therapy should be initiated when the patient has good performance status, no to minimal symptoms, and evidence of disease progression within the last 6 to 12 months. Patients who are symptomatic from their disease need systemic therapy.
The MKIs vandetanib and cabozantinib offer meaningful therapeutic options for MTC. Vandetanib was approved as a result of a phase 3 trial that met its primary end point of PFS [Wells SA et al. J Clin Oncol. 2012]. Patients with a RET mutation, particularly the M918T mutation, had a tremendous benefit from vandetanib. Vandetanib has a black box warning about QTc prolongation that occurred in 8% of patients who received it.
Cabozantinib is also approved for MTC, based on a phase 3 trial [Elisei R et al. J Clin Oncol. 2013]. Among 219 patients who received cabozantinib, 94% showed target lesion regression, whereas 27% of the 111 patients receiving placebo had target lesion regression. The median PFS was 11.2 months for cabozantinib vs 4.0 months for placebo (HR, 0.28; 95% CI, 0.19 to 0.40; P < .001). Patients with the RET M918T mutation had a prolonged PFS relative to patients with other RET mutations (HR, 0.15; 95% CI, 0.08 to 0.28) [Sherman SI et al. ASCO. 2013]. Patients with RAS mutations also benefited from cabozantinib.
Maria E. Cabanillas, MD, University of Texas MD Anderson Cancer Center, Houston, Texas, USA, discussed evidence to support salvage therapy after failure of a first-line kinase inhibitor in advanced thyroid cancer.
A retrospective review of adult patients with metastatic DTC found that median OS was 24 months for patients treated with sorafenib alone (n = 35) and 63 months for those receiving salvage therapy (n = 25; P = .013) [Dadu R et al. J Clin Endocrinol Metab. 2014]. PFS was 7.4 months (n = 15; 95% CI, 3.1 to 11.3) for all patients treated with sorafenib, and PFS was 11.3 months (n = 17; 95% CI, 5.3 to 24.4) for salvage therapy.
A phase 3 study of lenvatinib vs placebo in DTC found that patients who were TKI-naïve had a PFS of 18.7 months with lenvatinib treatment (n = 229; 95% CI, 16.4 to not estimable), while TKI-pretreated patients had a PFS of 15.1 months (n = 93; 95% CI, 8.8 to not estimable) [Schlumberger M et al. N Engl J Med. 2015].
A phase 2 trial of vemurafenib in patients with papillary thyroid cancer found that vascular endothelial growth factor receptor-2 inhibitor (VEGFR2i)-naïve patients (n = 9) had a PR rate of 35%, median PFS of 15.6 months (95% CI, 11.2 to not reported), and OS not reached [Brose MS et al. Eur J Cancer. 2013; (abstr 28)]. The VEGFR2i-pretreated patients (n = 6) had a PR rate of 29%, median PFS of 6.3 months (95% CI, 5.39 to not reported), and median OS of 9.8 months (95% CI, 7.39 to not reached).
A phase 1 study of cabozantinib in DTC found that patients previously treated with a VEGF pathway inhibitor still responded to cabozantinib [Cabanillas ME et al. Thyroid. 2014].
In MTC, very little evidence exists for salvage therapy. A phase 3 trial comparing cabozantinib vs placebo in 330 patients with metastatic MTC found that 43% of previously treated patients (19 of 44 patients) achieved a PR with cabozantinib [Elisei R et al. J Clin Oncol. 2013]. A retrospective study found that changing to a different, but similar, TKI in MTC yielded responses that were quite variable with a brief median time to failure [Weitzman SP et al. ENDO. 2015].
Recent trials and drug approvals have led to new options for advanced DTC and advanced MTC. Salvage therapy can benefit patients whose first-line TKI has failed, with greater evidence of benefit in DTC than MTC.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.