

Summary
Results from a propensity-matched cohort study suggest that long-term outcomes for patients with stage I non–small cell lung cancer may be superior with surgery than with stereotactic body radiation therapy.
- stage I non–small cell lung cancer
- NSCLC
- stereotactic body radiation therapy
- stereotactic ablative radiation therapy
- SBRT
- SABR
- propensity-matched cohort study
- oncology clinical trials
Surgical resection is the primary approach to the treatment of stage I non–small cell lung cancer (NSCLC). American College of Chest Physicians evidence-based guidelines [Howington JA et al. Chest. 2013] recommend the use of a minimally invasive surgical approach such as video-assisted thoracoscopic surgery (VATS) lobectomy in stage I disease. Nonsurgical approaches such as stereotactic body radiation therapy (SBRT), also known as stereotactic ablative radiation therapy (SABR), may offer an alternative to surgery. No prospective randomized trials comparing surgery with SBRT have been published.
Gaetano Rocco, MD, National Cancer Institute, Pascale Foundation, Naples, Italy, discussed a poster by Sahar Mokhles, MD, Erasmus University Medical Center, Rotterdam, the Netherlands, reporting the results of a retrospective, propensity-score matching cohort study that compared clinical outcomes in patients with stage I NSCLC treated with surgery (VATS lobectomy or thoracotomy) vs SBRT [Mokhles S et al. Ann Oncol. 2015], with a primary outcome of overall survival. Propensity-score matching, where a propensity score difference of 0.20 was used as the maximum caliper width, generated a cohort of 73 patients treated with surgery and 73 treated with SBRT.
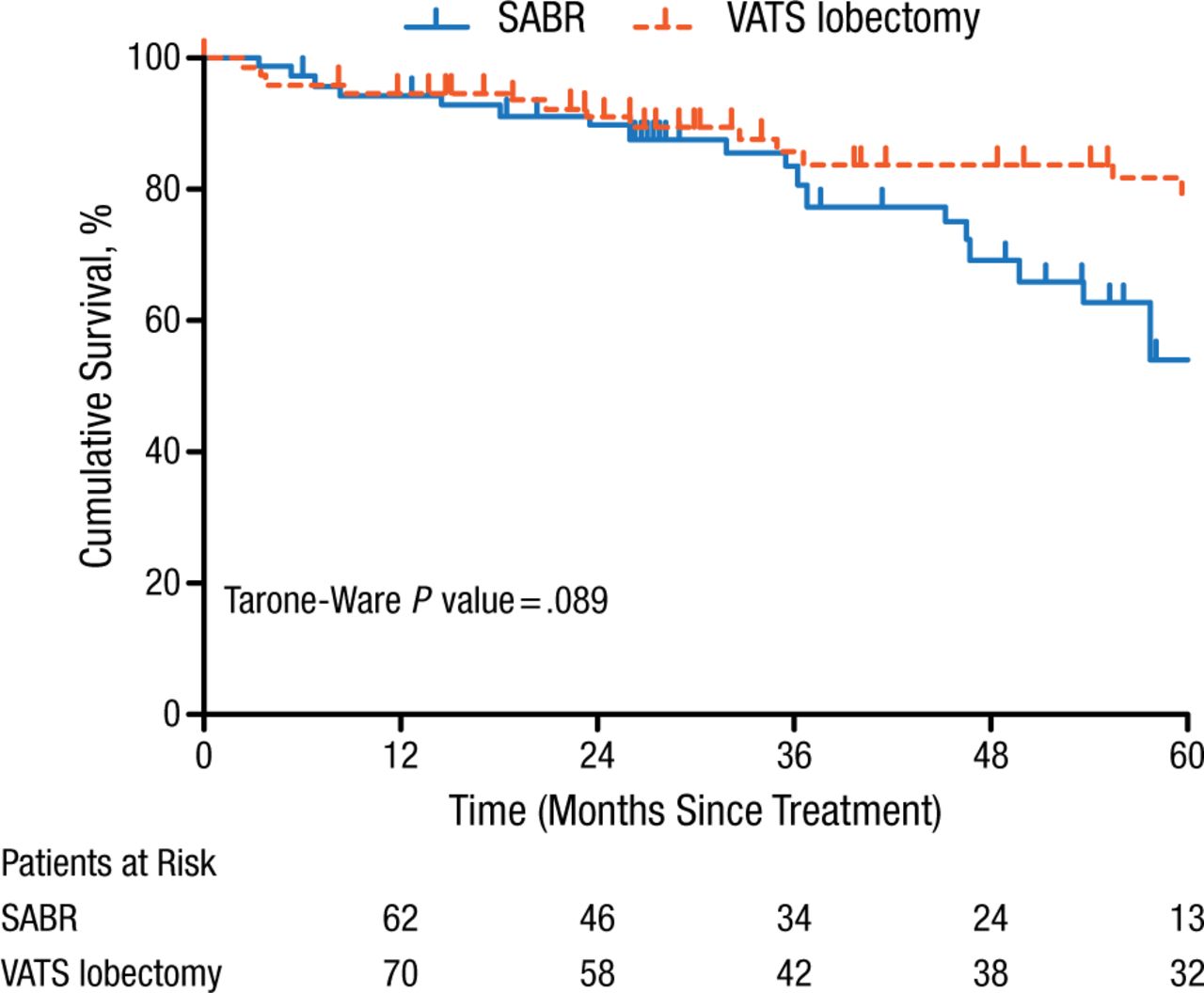
Median follow-up was 49 months for the surgery group and 28 months for the SBRT group; to correct for differences in follow-up time, the investigators compared survival curves using the Tarone-Ware test. Overall survival in the surgery group was 95% at 1 year and 80% at 5 years, compared with 94% at 1 year and 53% at 5 years in the SBRT group (P = .089; Figure 1). Although the survival difference between the 2 groups was not statistically significant, after 3 years there seemed to be better survival in surgically treated patients.
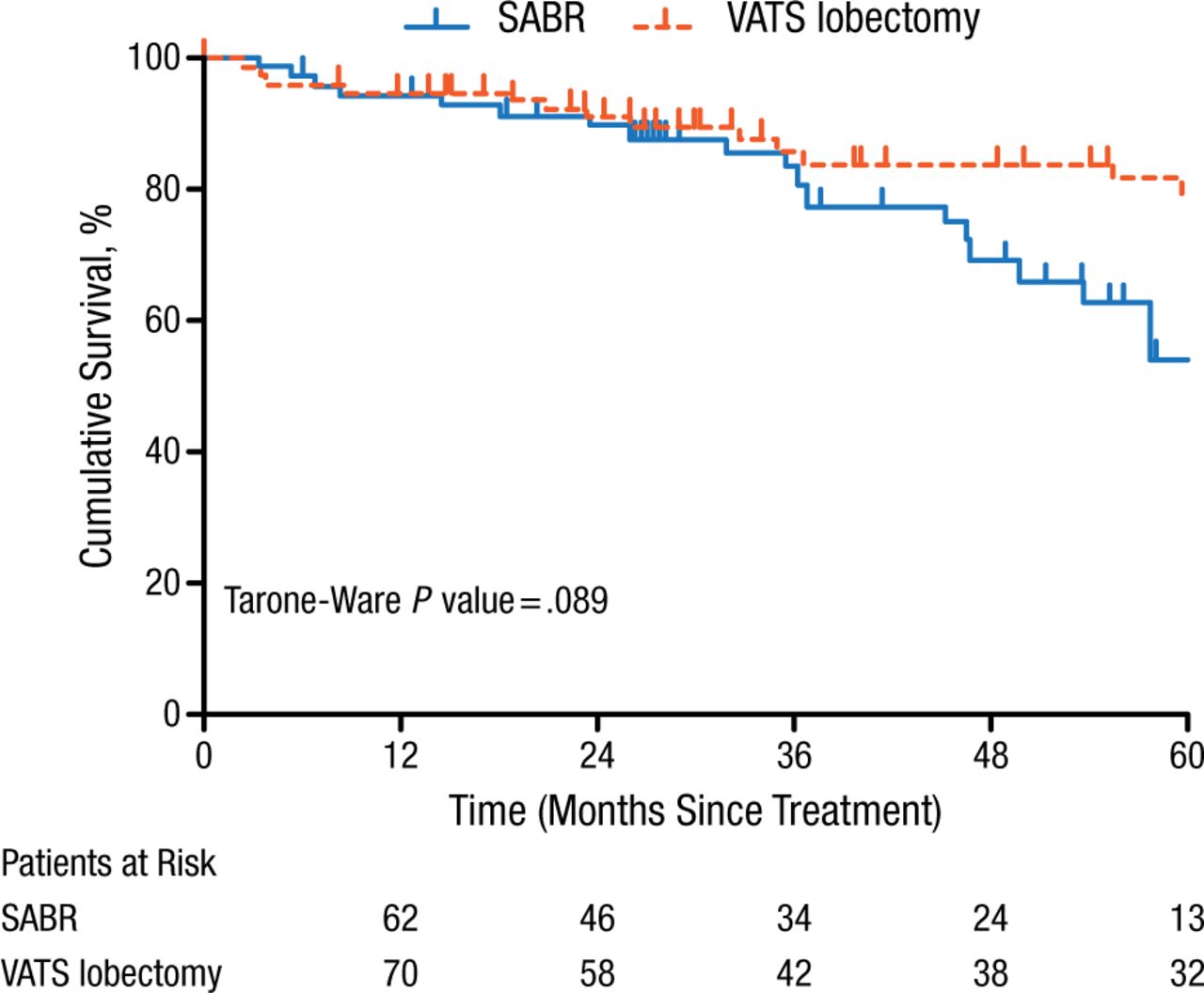
Cumulative Survival in Patients With Stage I NSCLC After Surgery or SABR
NSCLC, non–small cell lung cancer; SABR, stereotactic ablative radiation therapy; VATS, video-assisted thoracoscopic surgery.
Reproduced with permission from S Mokhles, MD.
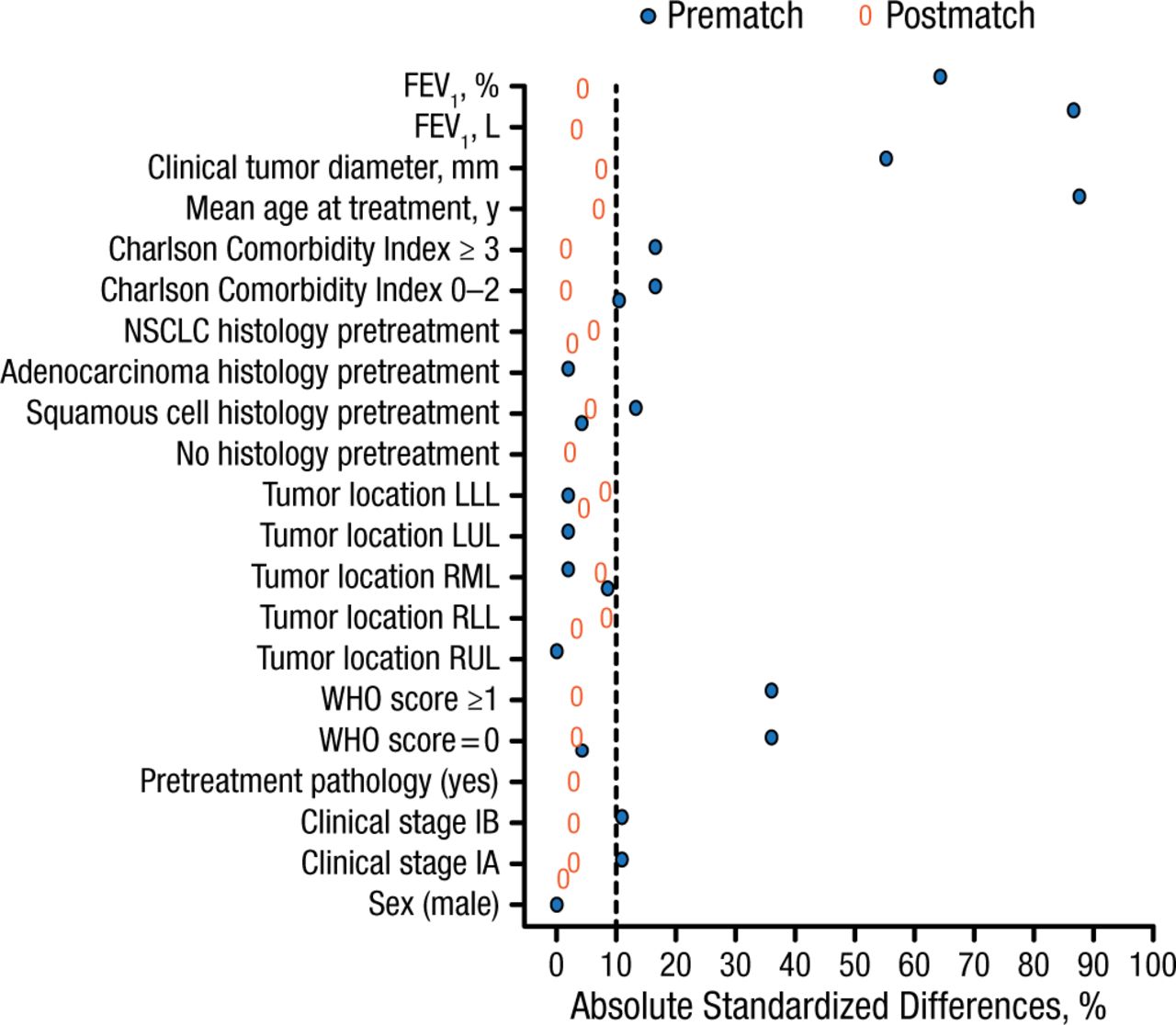
Absolute standardized differences for measure covariates were assessed to evaluate covariate balance across the groups, with results visualized using a Love-plot (Figure 2).
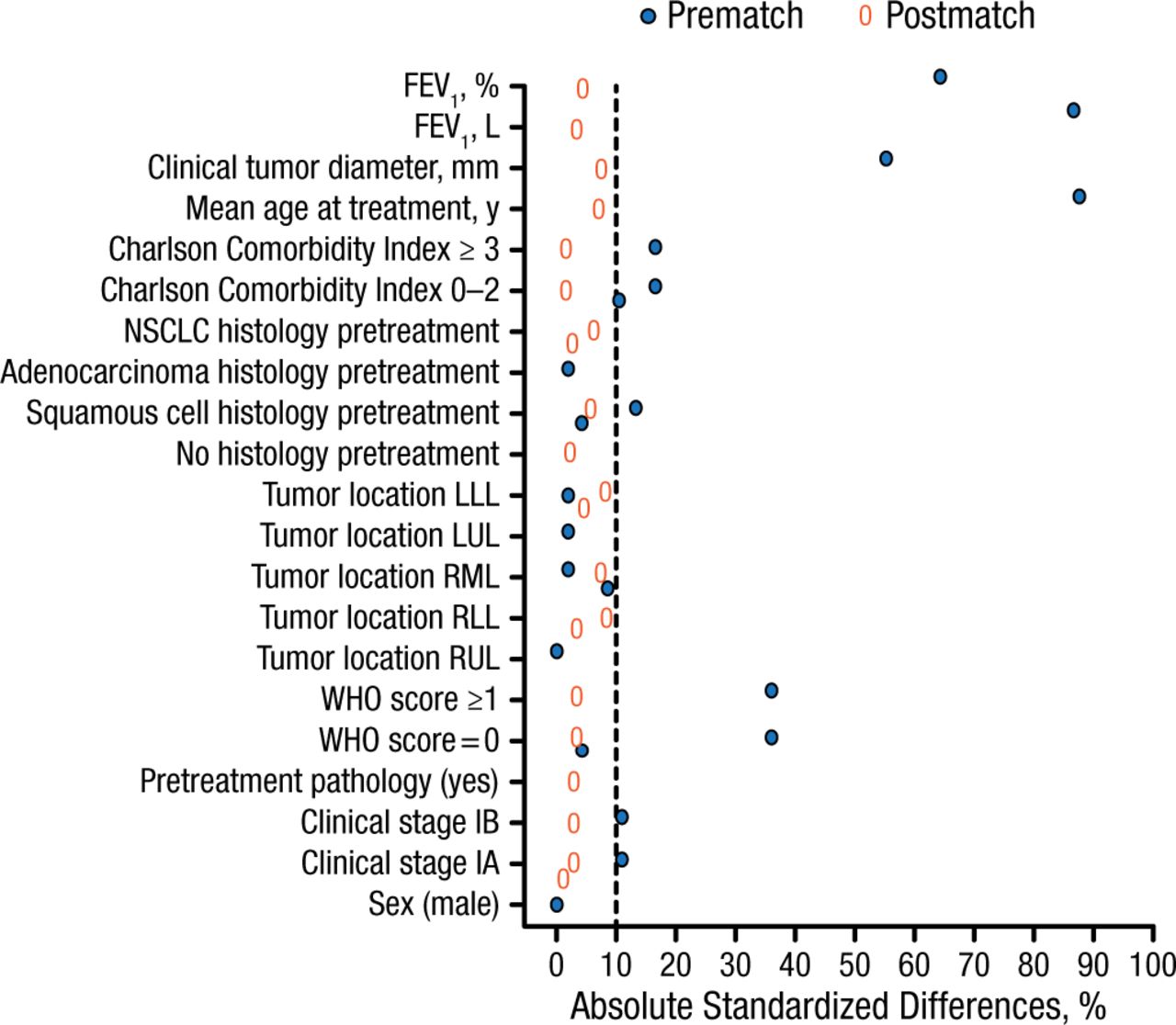
Love Plot for Baseline Covariates Between Surgery and SABR Groups
FEV1, forced expiratory volume in the first second of expiration; LLL, left lower lobe; LUL, left upper lobe; NSCLC, non–small cell lung cancer; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe; SABR, stereotactic ablative radiation therapy; WHO, World Health Organization.
Reproduced with permission from S Mokhles, MD.
Prof Rocco further discussed the grouping together of patients undergoing VATS lobectomy and SBRT, noting that these patient groups can have different results. He mentioned a recently published retrospective comparison of long-term outcomes in a single-center cohort of propensity-matched patients with stage I NSCLC who were treated with either VATS lobectomy (n = 41) or SBRT (n = 41) [Hamaji M et al. Ann Thorac Surg. 2015], in which survival rates varied significantly.
In response to questions posed by Prof Rocco and other discussants, Dr Mokhles, author of the poster under discussion, stated that 57% of surgically treated patients in the propensity-matched cohort and 74% of those treated with SBRT had T1 disease. Because the pathologic stage was not known for patients treated with SBRT, no concordance rate by pathologic stage could be established between the 2 groups. Every recurrence was confirmed with biopsy or 18F fluorodeoxyglucose–positron emission tomographic (FDG-PET) imaging. Staging of disease in the SBRT group was generally performed by computed tomography or FDG-PET scanning rather than by endobronchial ultrasonography.
In conclusion, data from this propensity-matched cohort study showed a trend toward overall survival as greater with surgery than with SBRT in patients with stage I NSCLC. Prospective randomized clinical trials should further investigate the clinical outcomes with these 2 treatments.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.