

Summary
New approaches to malignant pleural mesothelioma are developing through increased knowledge of its genomic landscape that has informed treatment approaches through precision medicine. This session also discussed the roles of surgery and radiotherapy for mesothelioma.
- malignant pleural mesothelioma
- genetics
- pathology
- surgery
- asbestos
- BAP1 protein
- tumor markers
- treatment outcome
- combined modality therapy
- radiation therapy
- adjuvant/neoadjuvant therapy
Malignant pleural mesothelioma (MPM) is a disease of increasing concern in the developing world due to asbestos exposure. This session discussed current knowledge of its genomics, the roles of surgery and radiation therapy (RT), and treatment options.
Understanding the Mesothelioma Genome
MPM has fewer mutations than other types of lung cancer, explained Giorgio V. Scagliotti, MD, PhD, University of Torino, Torino, Italy. The 3 most common somatic aberrations that occur in MPM are cyclin-dependent kinase inhibitor 2A (about 80% of cases), neurofibromin 2 (NF2; about 60% of cases), and BRCA1-associated protein-1 (BAP1; about 21% of cases, more smokers) [Bott M et al. Nat Genet. 2011; Testa JR Nature Genetics. 2011].
The gene product of NF2 is Merlin, which acts as a tumor suppressor gene. When NF2 is deleted, the pathway is overactive and its downstream pathway involves a mechanistic target of rapamycin (mTOR). As a result, mTOR inhibitors have been investigated in MPM. As 50% to 60% of mesothelioma has an inactivation of Merlin, inhibiting focal adhesion kinase could have therapeutic potential in Merlin-null tumors, and cell lines have responded to defactinib.
Gene sequencing of MPM has found > 500 mutations in 490 genes, with the vast majority being missense mutations [Guo G et al. Cancer Res. 2015]. A frameshift study classified the tumor cell lines into 2 clusters (C1 and C2), with the only significant difference in genetic alterations between these groups in both MPM in culture and MPM tumor samples being related to BAP1 (P < .04) [de Reyniès A et al. Clin Cancer Res. 2014]. Variations in BAP1 were concentrated mainly in exon 13. The colony stimulating factor 1 receptor gene was found to be more common in MPM than in normal cells [Cioce M et al. Cell Death Dis. 2014].
As patients with mutated tumor protein p53 have a worse prognosis than other groups [van Oijen MG, Slootweg PJ. Clin Cancer Res. 2000] and PIK3CA mutations correlate with early disease progression, PI3K and mTOR inhibitors have been investigated [Hoda MA et al. J Thorac Oncol. 2011; Mikami I et al. Oncol Rep. 2010; López-Lago MA et al. Mol Cell Biol. 2009].
Thoracic Surgeon’s Evolving Role in MSM
The best survival in MSM occurs after multimodality treatment, explained Walter Weder, MD, University Hospital Zurich, Zurich, Switzerland. The main aim of surgery is macroscopic complete resection, through the 2 main procedures of extrapleural pneumonectomy (EPP) and pleurectomy/decortication (P/D) [Rice D. Ann Cardiothorac Surg. 2012].
A systematic review of EPP vs P/D found that morbidity data is difficult to compare because the procedures have heterogeneous definitions (Figure 1) [Cao C et al. Lung Cancer. 2014]. Perioperative mortality was lower (2.9%) with P/D than with EPP (6.8%; P = .02). Both surgeries should be performed at dedicated MPM centers with experienced staff.
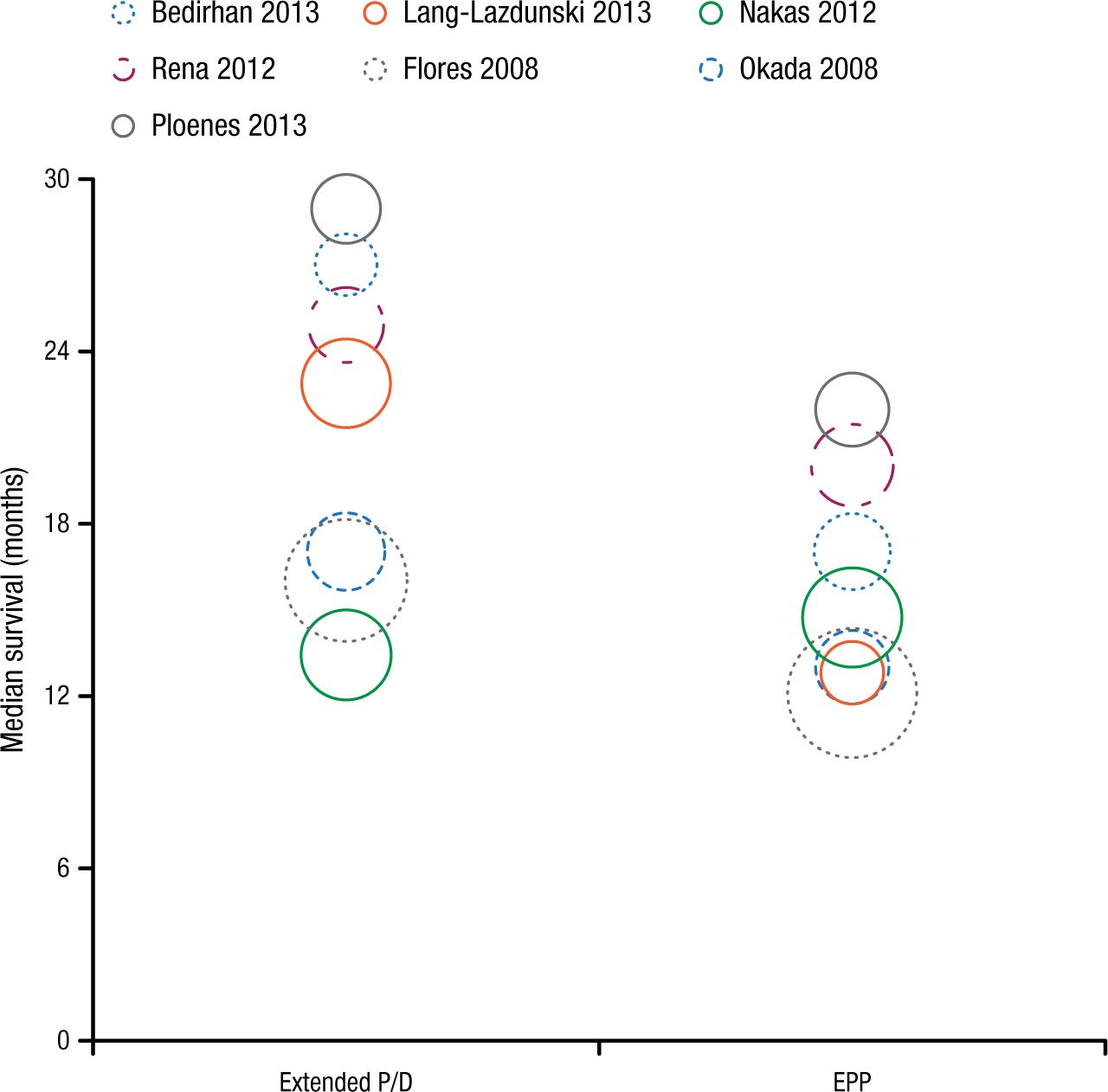
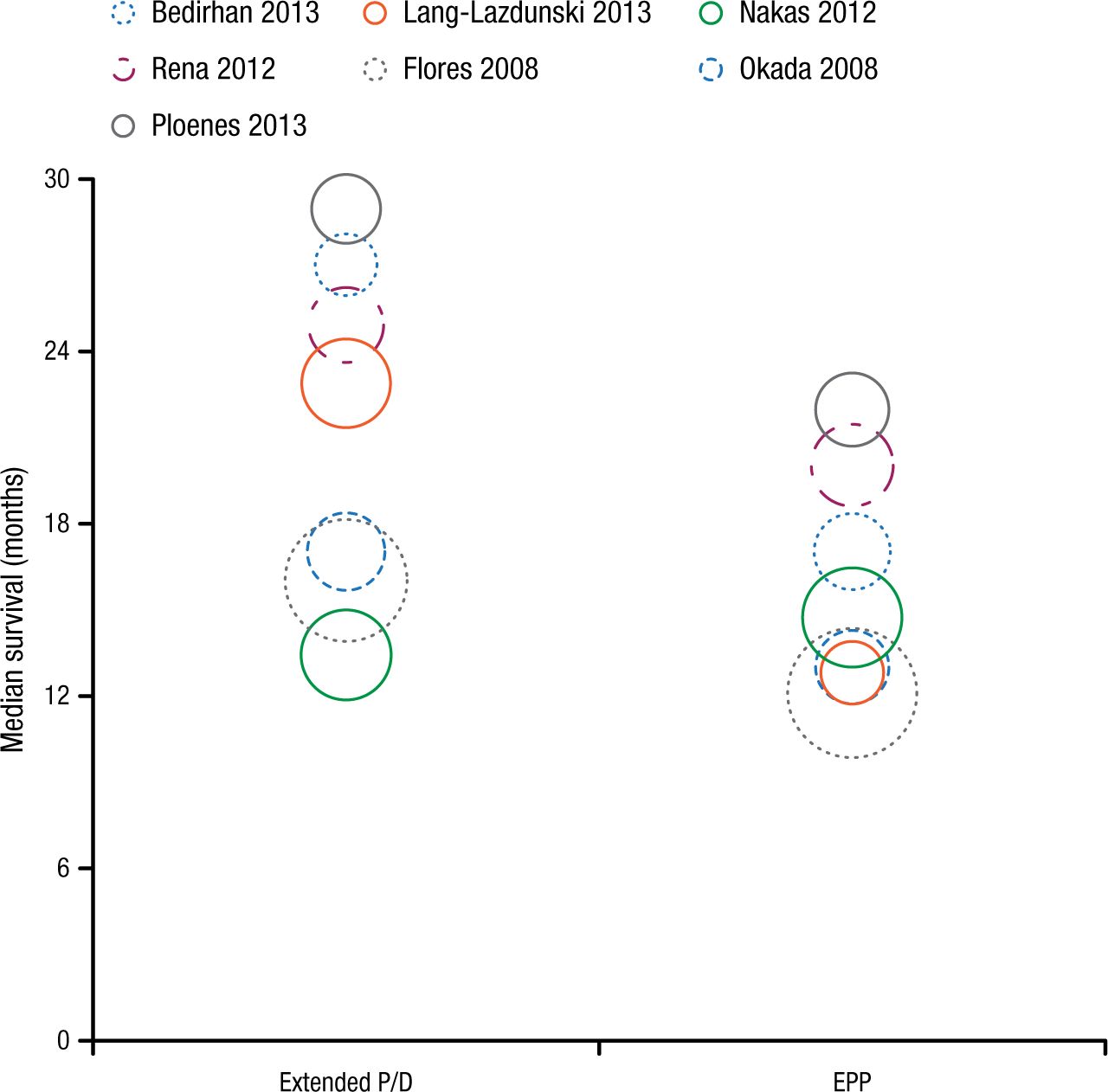
Meta-analysis of Median Survival and Surgery for MPM
Summary of median overall survival outcomes for patients with malignant pleural mesothelioma who underwent extended P/D or EPP. Circle radius is logistically proportional to the size of individual studies. Solid lines indicate survival measured from the date of diagnosis, and dotted lines indicate survival measured from the date of surgery.
EPP, extrapleural pneumonectomy; MPM, malignant pleural mesothelioma; P/D, pleurectomy/decortication.
Reprinted from Lung Cancer, Vol 83, Cao C et al, A systematic review and meta-analysis of surgical treatments for malignant pleural mesothelioma, Pages 240-5, Copyright (2013), with permission from Elsevier Ireland Ltd.
Currently, no standardized recommendation exists for surgery type. Preoperative functional assessment is mandatory, including pulmonary function and cardiac assessment. Considerations include performance status, patient desires, extent of tumor load, and adjuvant treatment plans. When macroscopic complete resection is deemed achievable, surgical cytoreduction is indicated [Rusch V et al. J Thorac Cardiovasc Surg. 2013]. MPM does not respond well to chemotherapy, though induction chemotherapy may allow for downstaging of the tumor and better resectability. However, induction chemotherapy increases surgical mortality and morbidity, and delaying surgery reduces resectability.
Adjuvant RT has an unclear benefit, though it may reduce local recurrences. Its challenges include the large target volume, nearby vital structures, and adverse events. Palliative RT may be used for pain control.
The Role of Radiation Therapy in Mesothelioma
RT for MPM is used in the palliative setting, in prophylaxis of port-site recurrence, and as an integral part of “curative” multimodality therapy for resectable disease. However, Umberto Ricardi, MD, University of Turin, Turin, Italy explained that little evidence supports the use of routine RT for MPM. Though RT is used in prophylaxis of port-site recurrence, systematic reviews have concluded that it did not influence the disease course [Chapman E, Garcia Dieguez M. Cochrane Database Syst Rev. 2010; Ung YC et al. Radiother Oncol. 2006]. Palliative RT is effective for pain control, as 47% of 30 patients evaluable at week 5 had pain improvement after RT [MacLeod N et al. J Thorac Oncol. 2015].
Adding RT, often combined with chemotherapy, after surgery improved median overall survival (OS) from 10.3 months to 20.1 months in a study of prognostic factors for 945 patients (P < .001) [Flores RM et al. J Thorac Oncol. 2007].
The use of intensity-modulated RT initially produced more fatal pneumonitis than 3D conformal RT. According to Prof Ricardi, if strict constraints are applied, 50 to 54 Gy post-EPP RT is feasible in well-selected patients affected with MPM (low toxicity burden).
Open questions remain on the selection of patients for trimodality treatment. After multimodality therapy for MPM, 75% developed a recurrence (118 of 158 evaluable patients) with a median follow-up of 83 months, 13.1 months to recurrence, and median survival of 15 months [Baldini EH et al. J Thorac Cardiovasc Surg. 2015], with local relapse in the homolateral hemithorax still representing the most typical pattern of relapse.
When patients are treated with EPP, it offers complete resection of all gross tumors and allows for the delivery of high-dose adjuvant hemithoracic RT, but it is linked with greater morbidity and mortality than lesser operations. Also, rapid progression of disease and limited life expectancy often occurs. The use of P/D is diffusively increasing, which often leads to equal or better outcomes than EPP [Hiddinga BI, van Meerbeeck JP. J Thorac Oncol. 2013].
P/D, as it is a less complete resection than EPP and has a higher risk for locoregional recurrence, poses a difficult problem for delivering RT, noted Prof Ricardi.
According to Prof Ricardi, pleural intensity-modulated RT, whether alone or after P/D, is feasible and safe, with delivered RT doses of 47 to 55 Gy and rates of grade 3 or higher toxicity of 20% to 30%. Adjuvant irradiation after P/D is not recommended outside clinical trials, which are ongoing.
Overall, MPM still has a dismal prognosis and it is unclear if any local treatment changes long-term survival. No local treatment has been found effective.
Old Drugs and New Approaches to Mesothelioma
Mesothelioma was previously considered a rare tumor, is asbestos related, is a public health issue in the developing world, has many diagnostic pitfalls, and has no validated curative treatment, said Paul Baas, MD, PhD, The Netherlands Cancer Institute, Amsterdam, The Netherlands. He explained the problems of mesothelioma studies, including that they take 2 to 8 years, which is too long; the population is heterogeneous in terms of previous treatments, stage and pathology, and measurable disease; the study setup is incomplete and lacks data on the impact of poststudy chemotherapy; and the number of translational studies is limited with no tumor assessments before or after treatment.
First-line treatment is chemotherapy, which provides symptom relief and increases OS. The standard is combining cisplatin and anti-folate, and it results in 80% of tumors recurring within 2 years and a median OS of 12 to 13 months, according to a 2003 study.
So far, novel and targeted agents have had no or very limited success. Amatuximab [Hassan R et al. Clin Cancer Res. 2014], thalidomide [Buikhuisen WA et al. Lancet Oncol. 2013], and vorinostat [Krug LM et al. Lancet Oncol. 2015] have failed or had minimal improvements. The PI3K-mTOR pathway is of interest to target in MPM. One recent study showed that 40% of cases express programmed death ligand [Mansfield AS et al. J Thorac Oncol. 2014], so immunotherapy is also of interest. Another approach is to test many drugs, including old ones, using a drug library to identify the best approach. The library includes histone deacetylase inhibitors, proteasome inhibitors, anthracyclines, and antineoplastic antibiotics.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.