

Summary
The current evidence for the optimal delivery of radiation therapy in patients with small cell lung cancer is reviewed in this article. Hippocampal avoidance prophylactic cranial irradiation is being studied to reduce the associated neurocognitive deficits. Thoracic radiation therapy combined with prophylactic cranial irradiation was shown to improve overall survival and progression-free survival and reduce intrathoracic progression in the CREST trial.
- CALGB 30610 trial
- CONVERT trial
- CREST trial
- hippocampal avoidance PCI
- neurocognitive toxicity
- prophylactic cranial irradiation
- radiation therapy
- small cell lung cancer
- neurocognitive toxicity
- oncology clinical trials
Small cell lung cancer (SCLC) is characterized by rapid tumor growth, initially high response rates to chemotherapy and radiation therapy (RT) followed by rapid treatment resistance, and about a 10% survival rate at 5 years. Different treatment approaches may be needed for different tumors, because experimental data have demonstrated a high level of cell heterogeneity, phenotypic variability, and a differential expression of epithelial-mesenchymal transition among different cell lines of SCLC, stated Rebecca Bütof, MD, University Hospital, TU Dresden, Dresden, Germany.
The optimal time to initiate RT appears to be early (within 30 days) after the start of chemotherapy. In part, this may be due to the accelerated repopulation of tumor cells that typically occurs after any cytotoxic therapy, noted Prof Bütof. Two meta-analyses showed a survival benefit with early vs late initiation of RT [Pijls-Johannesma M et al. Cancer Treat Rev. 2007; Fried DB et al. J Clin Oncol. 2004].
Regarding the optimal dose of RT, the total gross tumor volume was shown to be an independent prognostic factor for overall survival (OS) [Reymen B et al. Int J Radiat Oncol Biol Phys. 2013], thus volume-based dosing may be needed. Turrisi and colleagues showed in 1999 that twice-daily RT delivered over a shorter period of time (3 weeks, vs 5 weeks for once-daily RT) resulted in better median survival (23 months vs 19 months) and 5-year survival (26% vs 16%). Delivering RT in more (15) fractions was shown to improve 3-year OS vs conventional fractionation (39.4% vs 19.1%; P = .004) [Socha J et al. J BUON. 2015]. However, the results of the CALGB 30610 [NCT00632853] and CONVERT [NCT00433563] trials are awaited to provide definitive answers for the optimal timing, dosing, and fractionation for RT in SCLC. Research is also underway to develop RT techniques that will spare normal tissue to ultimately reduce side effects related to RT.
Prophylactic Cranial Irradiation in SCLC
Prophylactic cranial irradiation (PCI) became the standard of care to reduce the incidence of brain metastases (BMs) in patients with SCLC based on a meta-analysis showing that PCI prevented, rather than delayed, BMs [Aupérin A et al. N Engl J Med. 1999]. These findings were supported by the EORTC trial in patients with extensive-stage (ES) SCLC [Slotman B et al. N Engl J Med. 2007]. However, new data from a Japanese study in patients with ES-SCLC raise new questions about the use of PCI, because this study showed a higher incidence of BMs and no improvement in OS [Seto T et al. J Clin Oncol. 2014 (abstr 7503)].
Notably, the Japanese study used magnetic resonance imaging to define BMs, rather than symptomatic BMs as used previously. Yet, this trial was terminated early and the publication of the complete final results is needed to determine whether recommendations for the use of PCI should change, stated Cecile Le Péchoux, MD, Institut Gustave Roussy, Villejuif, France. Further, differences in patient selection and the use of more second-line treatment in the Japanese study may contribute to differences in results between the studies.
Neurocognitive toxicity is a concern with PCI, with reports of a higher risk of decline in self-reported cognitive functions at 6 and 12 months (P < .0001) and declines in recall on the Hopkins Verbal Learning Test (HVLT) at 6 and 12 months (P = .002) [Gondi V et al. Int J Radiat Oncol Biol Phys. 2013]. A significant decline in memory at 1 year was also reported [Sun A et al. J Clin Oncol. 2011].
Hippocampal avoidance (HA) when delivering whole brain RT was shown to preserve memory and quality of life in a study of this approach performed in 42 patients with lung or breast cancer who were compared with historical controls [Gondi V et al. J Clin Oncol. 2014]. The prospective, phase 3 HA-PCI trial [NCT01780675] is investigating the impact of this approach on the primary outcome of the total recall score of the HVLT at 4 months. A decline in this score of > 5 will be considered a failure, stated the lead investigator, Jose Belderbos, MD, PhD, The Netherlands Cancer Institute, Amsterdam, The Netherlands. RT will be delivered in 10 fractions up to 25 Gy, and magnetic resonance imaging will be performed at baseline, 4 months, and 1 year. Neurocognitive function, quality of life, incidence of BMs, and survival will also be assessed.
Thoracic Radiation Therapy for ES-SCLC
Recent data from the CREST trial [Slotman BJ et al. Lancet. 2015] provide more support for the use of thoracic radiation therapy (TRT) to treat residual intrathoracic disease in patients with ES-SCLC who have undergone chemotherapy and PCI. A retrospective study [Zhu H et al. Cancer. 2011] and an older single-center study by Jeremic and colleagues had shown improved OS with TRT.
Ben Slotman, MD, VU University Medical Center, Amsterdam, The Netherlands, explained that patients were randomized to PCI plus TRT or to PCI alone, with study treatment to begin between 2 and 7 weeks after chemotherapy ended. In the intention-to-treat analysis, there were 247 patients in the PCI plus TRT arm and 248 patients in the PCI arm. The median age was 63 years, 10.5% had a WHO performance score of 2, and 88% had persistent intrathoracic disease. The response to platinum-based chemotherapy was complete in 5%, partial in 70%, and good in 24%.
The difference in OS at 1 year did not reach statistical significance between the 2 groups (HR, 0.84; 95% CI, 0.69 to 1.01; P = .066). However, at 2 years, OS was greater with PCI plus TRT vs PCI alone (13% vs 3%; P = .004). Progression-free survival (PFS) was also significantly improved with PCI plus TRT (HR, 0.73; 95% CI, 0.61 to 0.87; P = .001).
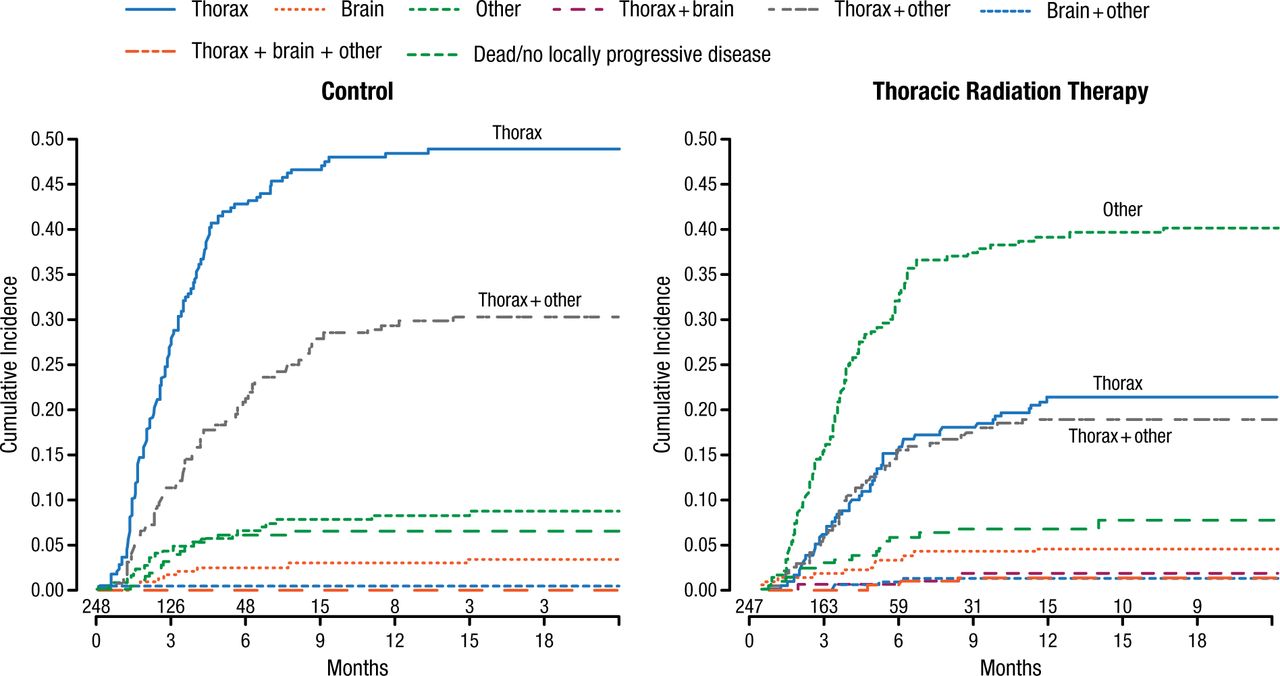
In patients with residual intrathoracic disease vs those without, there was a significant improvement with TRT for OS (HR, 0.81; 95% CI, 0.66 to 1.00; P < .05) and PFS (HR, 0.70; 95% CI, 0.70 to 0.85; P = .002). Notably, there was a lower risk of disease progression within the thorax compared with other sites in the PCI plus TRT arm vs PCI alone (Figure 1).
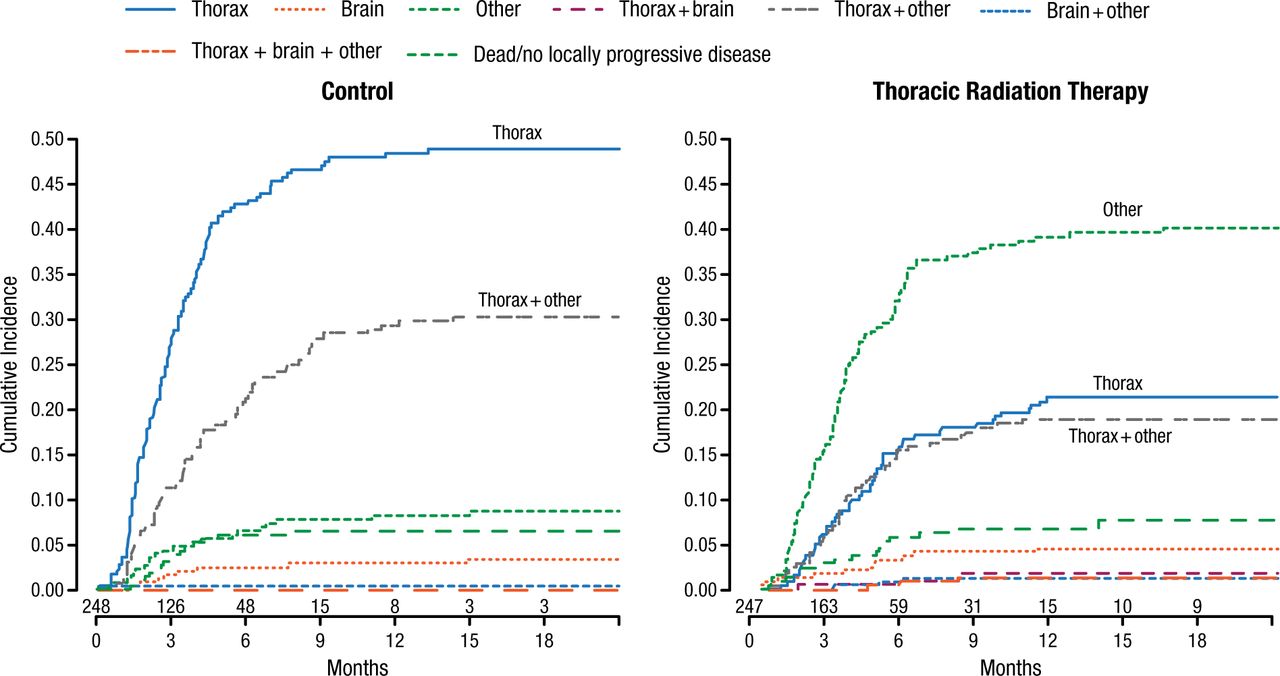
Site of First Relapse in the CREST Trial
Reproduced with permission from B Slotman, MD.
Regarding the CREST trial not meeting its primary end point at 1 year, Prof Slotman stated it should have been a 2-year trial, because a meta-analysis by Pignon and colleagues showed that a survival benefit with TRT was not seen until 2 years. Furthermore, there continues to be about a 40% risk of disease progression in this population, and continued research is needed.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.