

Summary
Osteochondral lesions of the talus can be repaired using bone marrow stimulation. However, clinical outcomes may be less than desirable in older patients or those with very large defects. Direct injection of mesenchymal stem cells as an adjunct to bone marrow stimulation may offer a reasonable alternative for these patients.
- talus
- osteochondral lesions
- bone marrow stimulation
- mesenchymal stem cells
- foot & ankle conditions
Osteochondral lesions of the talus (OLTs) are injuries to the talus that involve both the bone and the overlying articular cartilage. These lesions can occur after a single traumatic injury or as a result of repeated trauma; common symptoms include prolonged pain, swelling, catching, and/or instability of the ankle joint. While the exact incidence of symptomatic OLTs is unknown, they are a significant source of ankle morbidity.
While many OLTs can be treated nonoperatively, there are a number of available options for patients who require surgery, including bone marrow stimulation (BMS). Stimulation of the bone marrow results in the recruitment of mesenchymal stem cells (MSCs). These cells initiate an inflammatory response, subsequent release of cytokines and growth factors, and stimulation of tissue healing that then fills in the cartilage defect with fibrocartilage [Walther M et al. Oper Orthop Traumatol. 2014]. However, there is some controversy as to which patients are optimal candidates for BMS, as data suggest that patients who are older or have larger defects may experience less desirable outcomes [Chuckpaiwong B et al. Arthroscopy. 2008]. Therefore, there is some interest in learning whether these patients would be better served by an injection of MSCs directly into the OLT alongside BMS.
To further elucidate that hypothesis, Yong Sang Kim, MD, Yonsei Sarang Hospital, Seoul, Republic of Korea, presented data from a study designed to compare clinical and radiographic outcomes between 2 groups of patients with OLT. One group received an MSC injection as an adjunct to BMS; the other group underwent BMS alone (conventional group). There were no significant differences between the 2 groups relative to baseline characteristics or follow-up times (Table 1).
Comparison of the 2 Groups
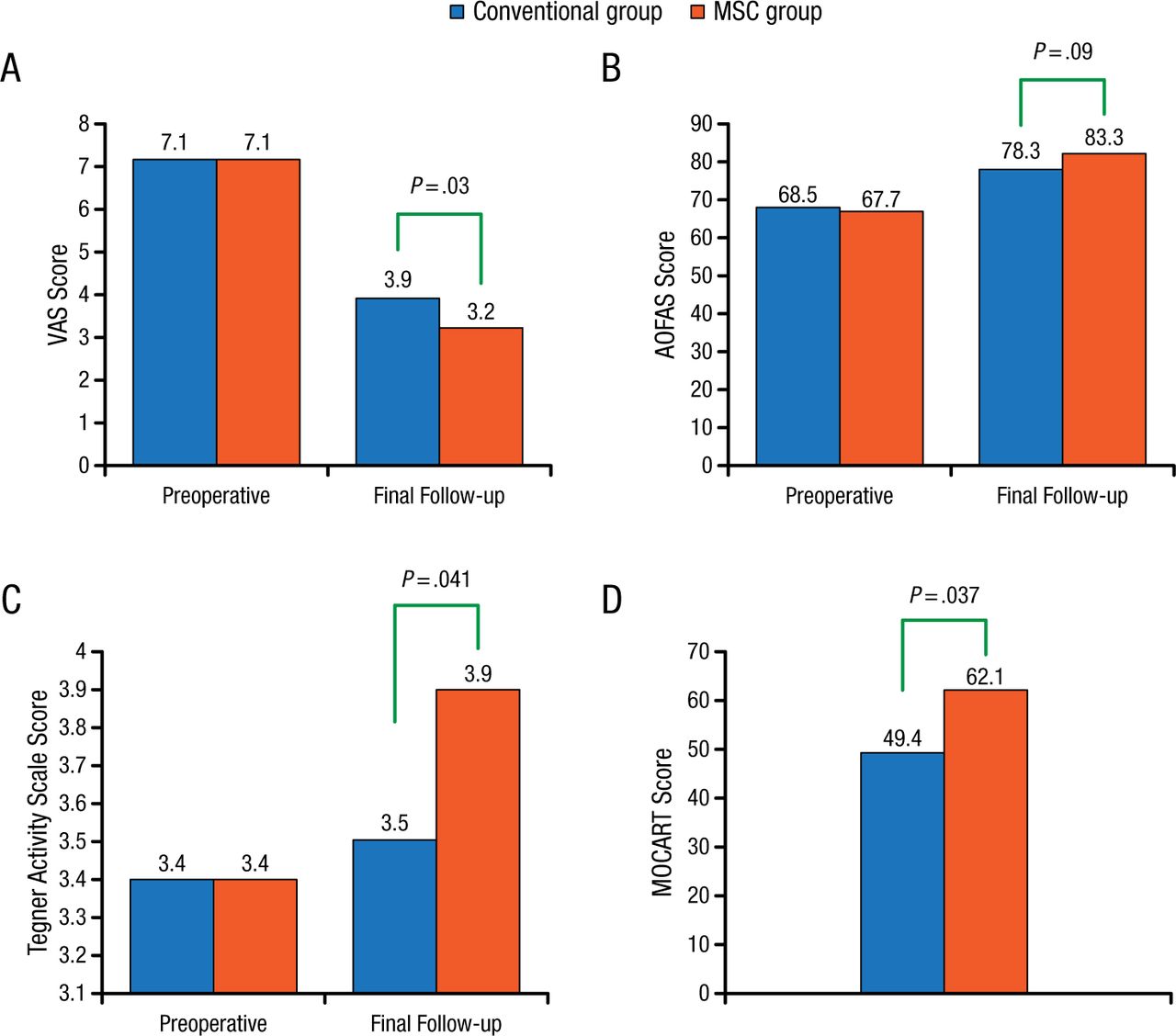
Three measures were used to evaluate clinical outcomes: the visual analog scale for pain, the American Orthopaedic Foot & Ankle Society Ankle-Hindfoot Scale, and the Tegner Activity Scale. The Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score measured radiographic evaluations.
In both groups, improvements were noted in all 3 clinical outcomes as well as the radiographic outcome. All clinical and imaging outcomes improved significantly in the MSC group compared with the conventional group (Figure 1).
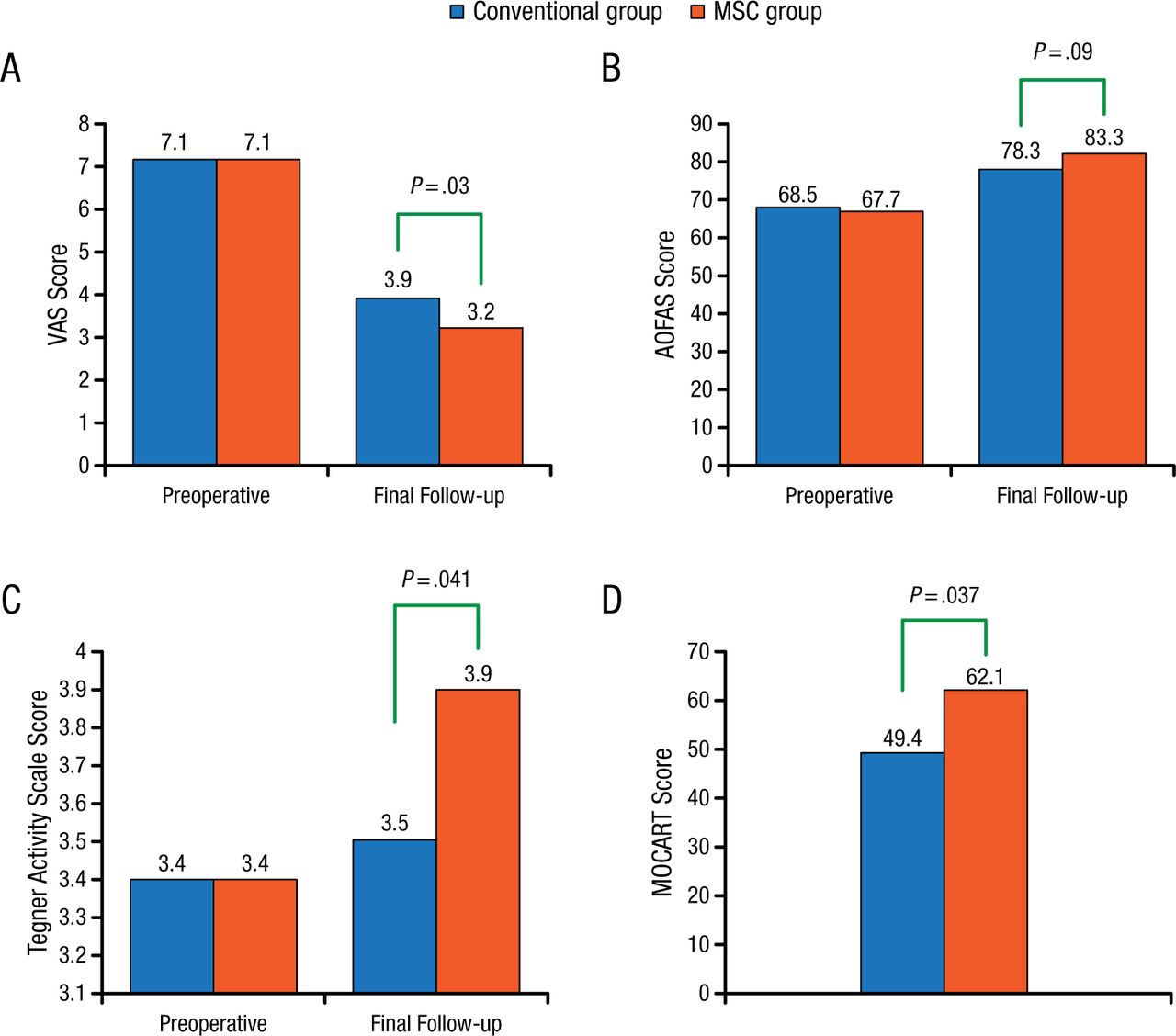
Improvements in Clinical and Radiographic Outcomes
AOFAS, American Orthopaedic Foot & Ankle Society; MOCART, Magnetic Resonance Observation of Cartilage Repair Tissue; MSC, mesenchymal stem cell; VAS, visual analog scale. Reproduced with permission from YS Kim, MD.
There was a significant correlation between the MOCART score and clinical outcomes in both groups (P < .05). Patient age (≥ 46.1 years), larger lesion size (≥ 151.2 mm2), and the presence of a subchondral cyst were all associated with worse MOCART scores in the conventional group (P = .015, .004, and .013, respectively) but not in the MSC group.
Prof Kim summarized these findings as encouraging and suggested that injection of MSCs alongside BMS might be an additional therapeutic option for patients with OLT who are likely to have a poor prognosis with BMS alone.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.