

Summary
In this hands-on, case-based session, 4 orthopedic surgeons presented clinical pearls and case studies that illustrated complex knee injuries in high-level athletes, diagnosis and management of injuries to the posterolateral corner, factors affecting knee reconstruction of the morbidly obese, and reconstruction of the anterior cruciate ligament.
- anterior cruciate ligament
- ACL
- posterolateral corner
- PLC
- posterior collateral ligament
- PCL
- knee
- multiligament
- obesity
- injury
- dislocation
- orthopaedics & sports medicine clinical trials
- hip & knee conditions
- orthopaedic procedures
- sports medicine
- trauma
There is much controversy regarding the ideal management of the dislocated knee, with ongoing debate regarding surgical vs nonsurgical management, allografting vs autografting, repair vs reconstruction, and the optimal time to surgical repair following the initial injury [Fanelli GC et al. Instr Course Lect. 2011].
In a symposium designed to address these challenging issues, 4 speakers presented case studies and clinical techniques that illustrated best practices in managing complex knee injuries in different populations using several different surgical approaches.
Joel Boyd, MD, TRIA Orthopaedic Center, Bloomington, Minnesota, USA, began the session by reviewing a case study of a high-performance 24-year-old soccer player who sustained a slide tackle injury to the medial side of the right leg 5 days prior to her medical visit. She complained of swelling, pain, instability, and an inability to dorsiflex her right foot. Physical examination findings included
2+ effusion,
2+ Lachman test with no end point,
3+ posterior drawer,
varus laxity at 0° and 30°,
no active dorsiflexion, and
diminished sensation over the dorsum of the foot.
Magnetic resonance imaging (MRI) suggested rupture of the anterior and posterior cruciate ligaments (ACL and PCL, respectively) and tendon avulsion off the fibula head. Other MRI findings included attenuation of the popliteus tendon, a lateral capsular tear, a lateral gastrocnemius tendon avulsion off the femur, and a contusion of the medial femoral condyle bone.
Dr Boyd reviewed possible surgical options for this patient, which included a repair with or without augmentation using an internal brace with FiberTape or a soft tissue graft, a Larson loop, a modified Larson loop, or an anatomic reconstruction.
The patient subsequently underwent repair of the right knee lateral collateral ligament and biceps tendon with extracapsular reconstruction using allograft peroneal tendon (Larson loop). She also underwent reconstruction/augmentation of the anterolateral ligament (ALL) using an internal brace. The ALL was braced because of its role as an important internal rotatory stabilizer of the knee, especially in flexion angles between 30° and 60° [Claes SA et al. AAOS 2013 (abstr SE73)]. Of note is that PCL repair was not addressed at this time.
Postoperatively, she was stable to varus stress. Over time, she seemed to develop a soft end point to her ACL and still had PCL insufficiency along with peroneal nerve pain. The follow-up MRI 3 months later showed a stable ACL, allowing the surgeon to proceed with the plan to repair the PCL with augmentation of the ALL.
Dr Boyd used this case to illustrate that these procedures can safely be staged as > 1 procedure, that collateral damage should be addressed first, and that the central ligaments can be addressed 6 to 12 weeks after the collateral surgery.
The Challenges of ACL Reconstruction
As a follow-up to this case, Robert Marx, MD, Weill Cornell Medical College, New York, New York, USA, offered practical, step-by-step instruction to guide surgeons in successfully reconstructing the ACL.
According to Dr Marx, ACL reconstruction of a multiligament knee injury is complicated by the absence of the PCL, which makes arthroscopic orientation more challenging. In addition, ACL and PCL tunnels require an adequate bone bridge on the anterior tibial cortex so that the tunnels do not coalesce if transtibial PCL is attempted. With ACL and PCL reconstruction, there must be enough room for fixation of the medial collateral ligament on the proximal medial tibia, as there is a paucity of space available there.
Dr Marx reminded attendees that placement of the ACL tunnel on the tibia and femur can be more difficult with an absent PCL, and so surgeons must use anatomic landmarks and remain mindful of the orientation of the arthroscope. He cautioned that rotation of the arthroscope by just 10° to 20° can dramatically alter the position of the tunnels.
According to Dr Marx, planning the order of tunnel creation is key to a successful reconstruction. This is particularly important when building a bone bridge between the ACL and the PCL. If a transtibial PCL is performed, the pins should be placed 2 cm apart, which will create a 1-cm bone bridge after drilling. Because proper placement of the PCL tibial tunnel is critical to the success of the procedure, Dr Marx recommended that the ACL tibial pin be placed first; the pin should be left unreamed to avoid any fluid leaks. The PCL guide pin should be placed next and reamed before the ACL guide pin. If the PCL guide pin is inserted first, it may be too proximal and not allow for placement of the ACL pin and subsequent tunnel. After both guide pins are reamed over, the bone bridge is adequate to protect the tunnels from collapsing into each other after placement of interference screws.
After the first PCL tibial tunnel is created, Dr Marx then creates the femoral ACL socket to obtain optimal visualization. Last, the tibial ACL and femoral PCL tunnels are created. Fixation is performed after all the grafts are in and fixed on the femur. The PCL is done first with the knee at 90°, followed by the ACL in full extension, and, finally, the collaterals.
Dr Marx went on to recommend that double-bundle ACL reconstruction not be attempted in patients undergoing multiligament reconstruction, as it presents a risk of tunnel convergence. He also shared his surgical preference for metal screws, as they offer a better “bite” and are visible on x-ray. On the controversial topic of allograft vs autograft, Dr Marx reviewed data suggesting that, relative to PCL, one type is no better than the other [Hudgens JL et al. J Knee Surg. 2013]. However, for multiligament knee injury, he prefers to use all allograft because it avoids the risk of donor site morbidity.
“The Dark Side of the Knee”
In the past, the structure and function of the posterolateral corner (PLC) of the knee was poorly understood and dubbed by some as “the dark side of the knee.” However, recent advances in quantitative anatomy and biomechanics of this region of the knee have led to new reconstruction techniques and improved patient-based outcomes.
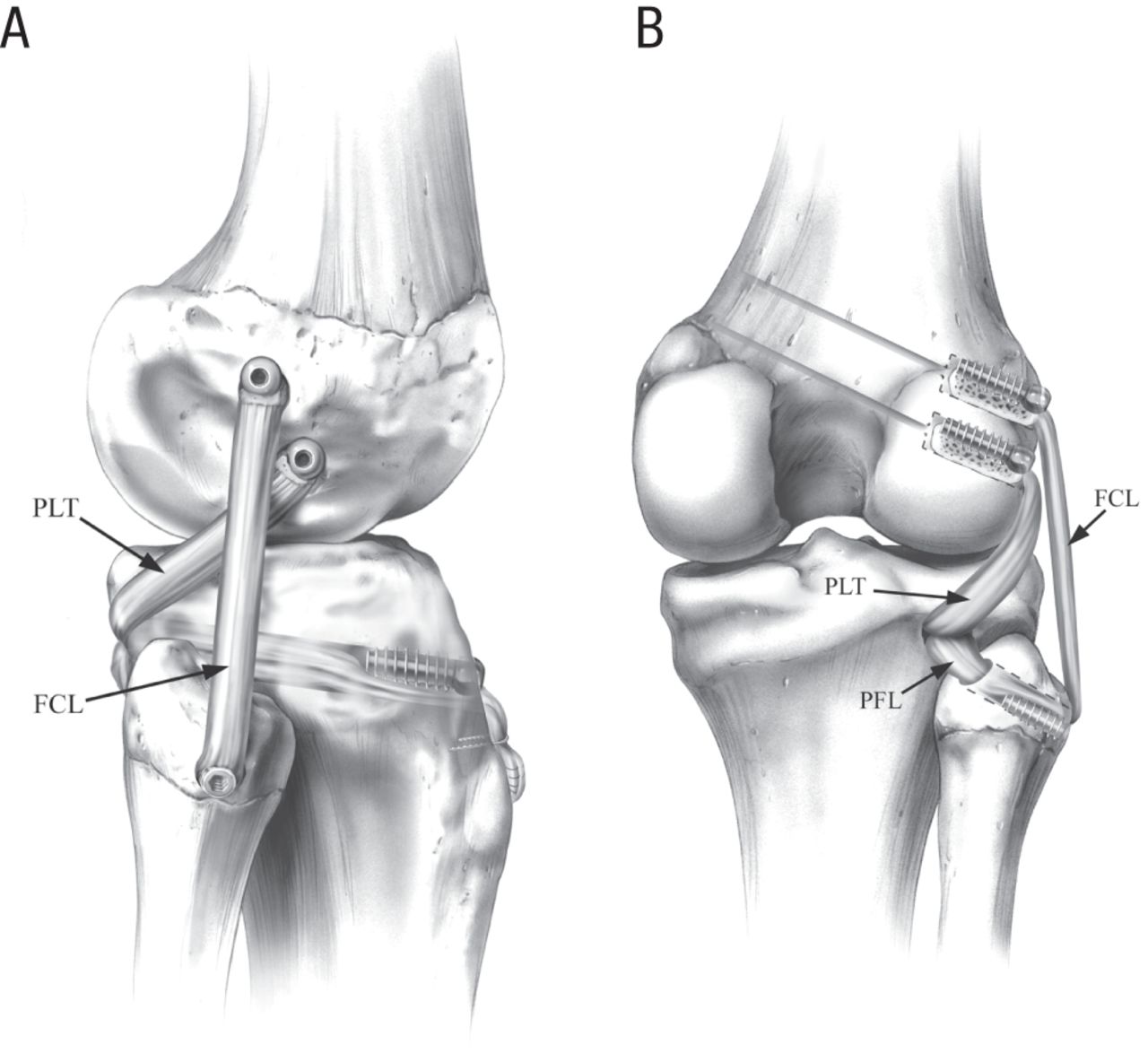
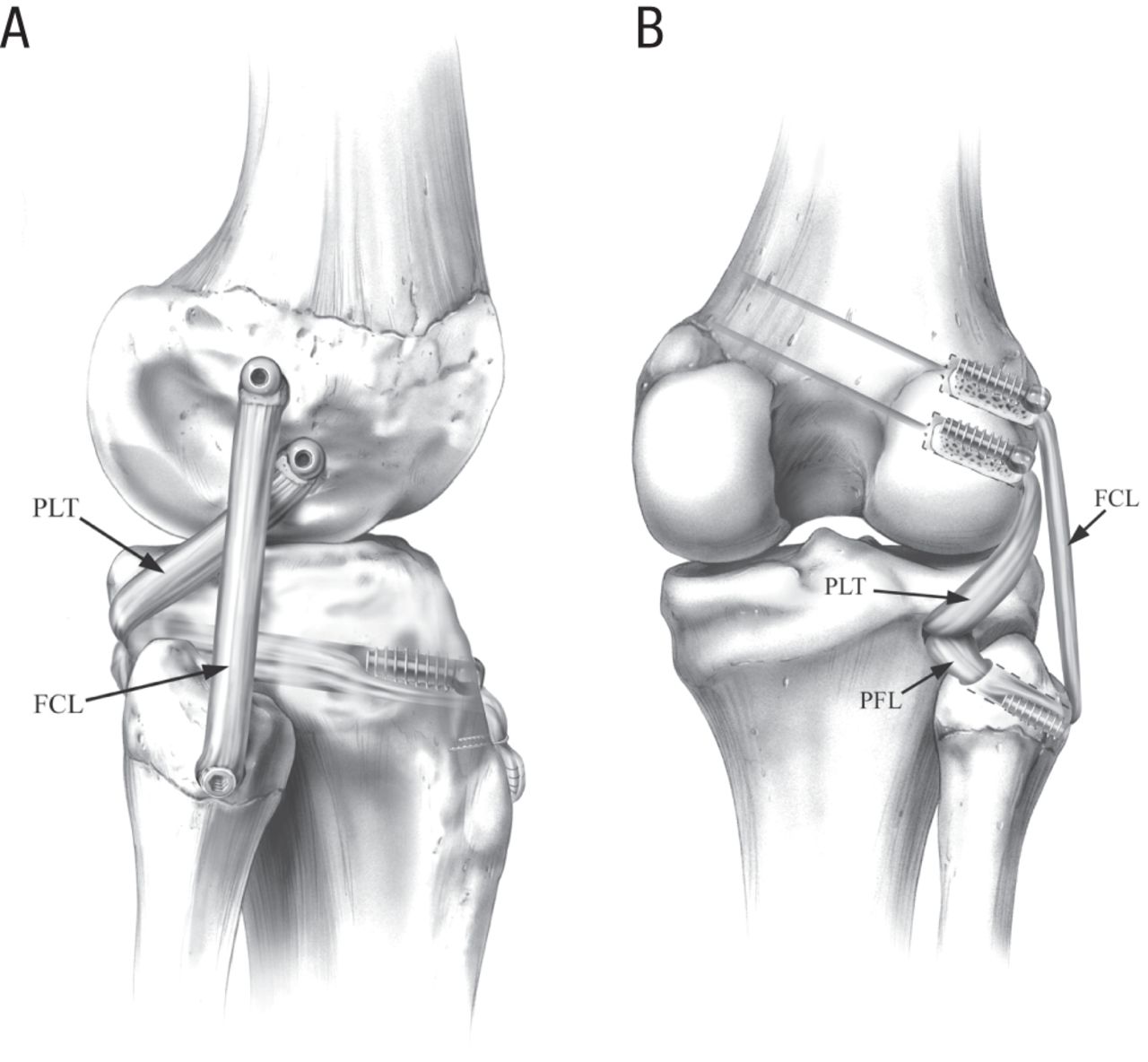
Robert LaPrade, MD, PhD, Steadman Philippon Research Institute, Vail, Colorado, USA, spoke of best practices in identifying and treating injuries of the PLC by repairing its 3 main stabilizing structures—the fibular collateral ligament, the popliteus tendon, and the popliteofibular ligament (Figure 1). According to Dr LaPrade, the ideal time for surgical repair of the PLC is within 2 to 3 weeks of the initial injury. If the knee is stiff, however, presurgical rehabilitation should be considered to improve range of motion. He recommended addressing all torn structures in 1 stage, rather than 2, because it is safe to do so and it allows patients to return to activities sooner. In addition, there is a definite risk of the first surgery failing if the cruciate ligaments are not concurrently reconstructed or vice versa. He also stressed the importance of preoperative planning, identifying the injury pattern by physical examination, MRI, and stress x-rays; choosing grafts; and preparing the surgical team so that tourniquet times can be kept between 90 and 120 minutes.
The Posterolateral Knee Reconstruction Procedure
FCL, fibular collateral ligament; PFL, popliteofibular ligament; PLT, popliteus tendon.
A, lateral view, right; B, posterior view, right.
LaPrade RF et al. Am J Sports Med (Vol. 32 No. 6), pp. 1405-1414, copyright © 2014. Reprinted by Permission of SAGE Publications.
Dr LaPrade then reviewed the 7 surgical steps to repair a complete tear of the PLC: (1) prepare a posteriorly placed skin flap using a lateral hockey stick incision; (2) perform a peroneal neurolysis at least 6 cm long, which includes the peroneus longus fascia; (3) prepare all tunnels at attachment sites; (4) address intra-articular pathology and fix cruciate grafts in the femur; (5) prepare the PLC grafts; (6) pass and fix the grafts; and (7) apply full range of motion on postoperative day 1.
Postreconstruction, patients should remain non-weight-bearing for 6 weeks. Dr LaPrade recommends early passive range of motion, trying to get from 0o to 90o on day 1. Patients can start on a stationary bicycle at postoperative week 7, with instructions to avoid isolated hamstring exercises for 4 months. Most patients who have a multiligament reconstruction can return to full activities at 9 to 12 months.
Managing the Morbidly Obese Patient
Mark Miller, MD, University of Virginia, Charlottesville, Virginia, USA, next spoke about the devastating effects of ultra-low velocity (ULV) multiligament injuries (MLIs) of the knee and the difficulty in managing these injuries in morbidly obese patients. While MLI dislocations are typically associated with high-velocity injuries, such as motor vehicle accidents or sports injuries, obese patients are at risk of MLIs from ULV injuries, such as simple falls that occur during activities of daily living [Azar FM et al. Am J Sports Med. 2011].
Dr Miller reviewed a study that evaluated the characteristics, risk factors, and complications associated with ULV dislocations of the knee [Werner BC et al. Am J Sports Med. 2014]. This was a 12-year retrospective chart review of 215 patients who had undergone operative treatment for MLI. Patients who suffered a ULV-MLI were significantly more likely to be morbidly obese and female and to develop peroneal and vascular injuries. Demographics and outcomes of the entire cohort are shown in Table 1.
Demographics and Outcomes of the MLI and ULV-MLI Cohorts
Overall, postoperative complications were significantly more common in the ULV-MLI group (Table 2).
Complications in the MLI and ULV-MLI Cohorts
Follow-up was available from 17 (70%) ULV-MLI patients at approximately 6 years, and 71% of the patients reported dissatisfaction with their surgical outcomes.
To improve functional outcomes and postoperative satisfaction among morbidly obese patients with a ULV-MLI, Dr Miller suggested the following:
Liberal use of rigid external fixation
Modify construct as needed
Delay cruciate reconstruction
Repair/reconstruct the PLC
Remove external fixation at 6 to 8 weeks
Work on range of motion
Lysis of adhesions, manipulation under anesthesia at 12 weeks as needed
Encourage weight loss and perhaps bariatric surgery
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.