

Summary
Prospective randomized data show significantly improved pain and function at 6 months for patients with osteoarthritis treated by intra-articular injections with either hyaluronic acid or platelet-rich plasma. Use of platelet-rich plasma may be more beneficial to treat active patients based on significant improvement in the International Knee Documentation Committee score.
- osteoarthritis
- hyaluronic acid
- platelet-rich plasma
- International Knee Documentation Committee
- visual analog scale
- Lysholm knee scale
- pain management
- orthopedic procedures
Emerging biochemical research suggests that platelet-rich plasma (PRP) is a biologic alternative to hyaluronic acid (HA) and may alter the intra-articular biologic environment in patients with osteoarthritis (OA) to help mitigate their symptoms [Chen WH et al. Biomaterials. 2014]. To examine this, Brian J. Cole, MD, Rush University Medical Center, Chicago, Illinois, USA, and colleagues conducted a double-blind, prospective, randomized clinical trial that compared the effects of PRP with HA for the treatment of OA in the knee. Patients with OA treated with intra-articular injections of either HA or PRP showed significant improvement in pain and function at 6 months. The study also showed that for active patients, PRP may be superior to HA, as suggested by a significant improvement in the International Knee Documentation Committee (IKDC) score.
The study included 111 patients (53 men; 58 women) randomized to either HA or PRP. The mean age of patients was 56.2 years. All patients had a minimum of 3 months of symptomatic unilateral knee OA and Kellgren–Lawrence grade 1 to 3 OA.
Patients in each treatment cohort received 3 weekly ultrasound-guided injections of their respective treatment (either HA or PRP). Following their index treatment, patients in each cohort were seen again and assessed at weeks 6, 12, and 24 by clinical examination and by completing a survey that included a number of measures: the Lysholm knee scale, the IKDC score, the Western Ontario and McMaster Universities Osteoarthritis Index, and the visual analog scale (VAS) for pain.
At these time intervals, as well as at 3- and 6-month follow-up, patients also underwent ultrasound-guided knee aspiration for synovial fluid analysis. Using an enzyme-linked immunosorbent assay, synovial fluid was grouped and analyzed for catabolic factors.
Of the 111 patients, 11 (9.9%) were lost to follow-up or were unwilling to complete the study.
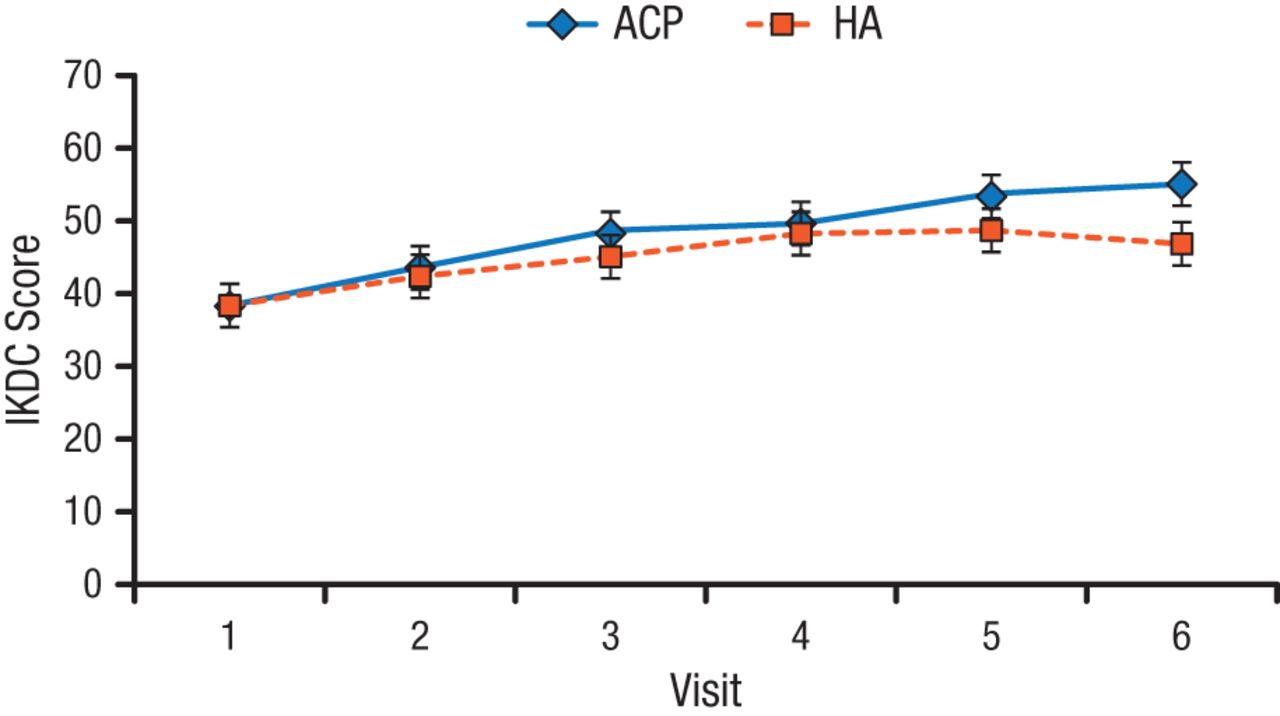
The study found that patients in both cohorts had a significant improvement from the index visit to 6 months after treatment based on all scales measured (P < .01). Patients who received PRP, however, showed a significantly higher IKDC score at 6 months compared with patients who received HA (P < .02; Figure 1). According to Dr Cole, the significant improvement in IKCD score suggests that PRP is superior to HA in active patients as this scoring system uses active participation in strenuous sports as its upper limit.
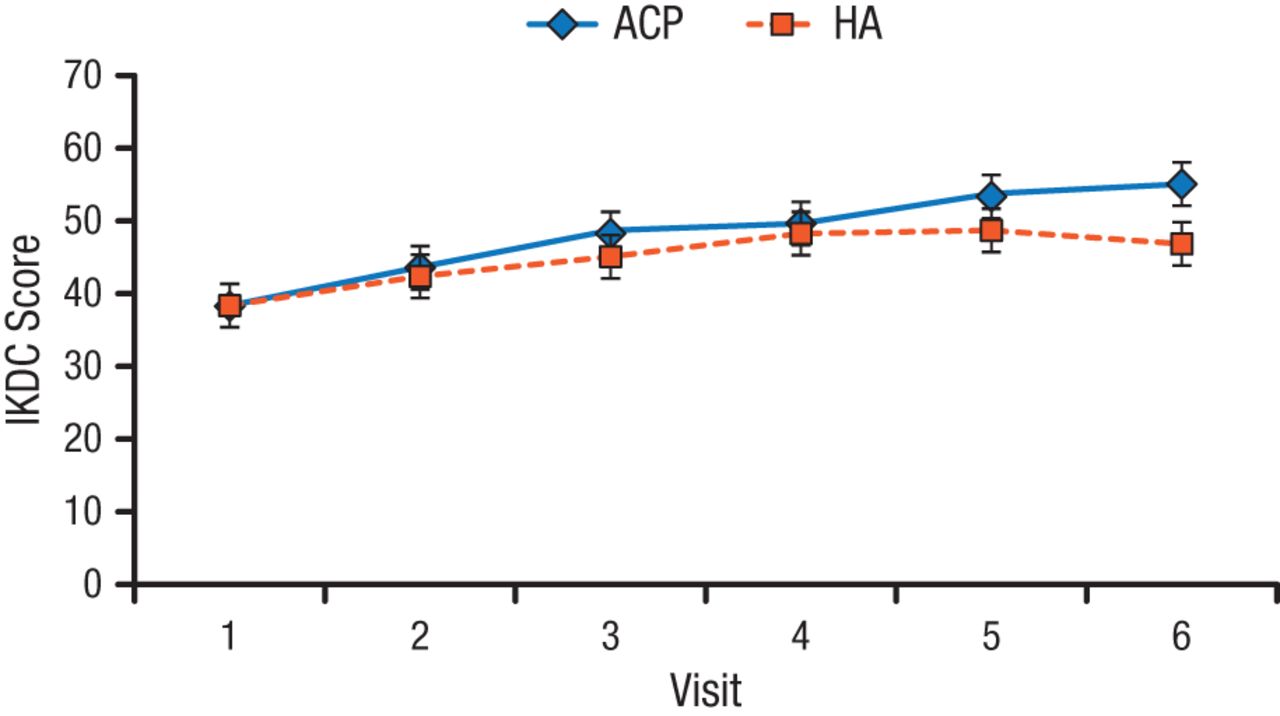
Higher IKDC Score in Patients Treated With PRP vs HA
ACP, autologous conditioned plasma; HA, hyaluronic acid; IKDC, International Knee Documentation Committee; PRP, platelet-rich plasma.
Reproduced with permission from BJ Cole, MD.
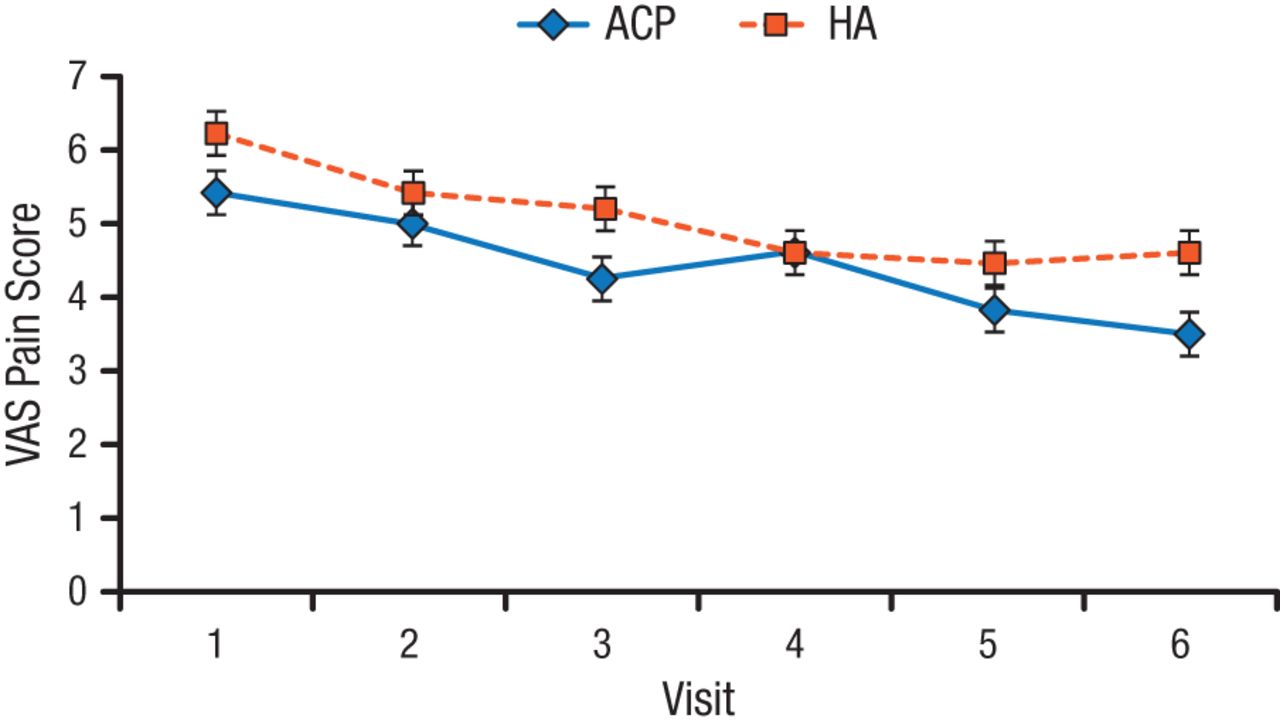
The study also found a significantly lower VAS pain score in patients treated with PRP compared with HA (P < .01; Figure 2).
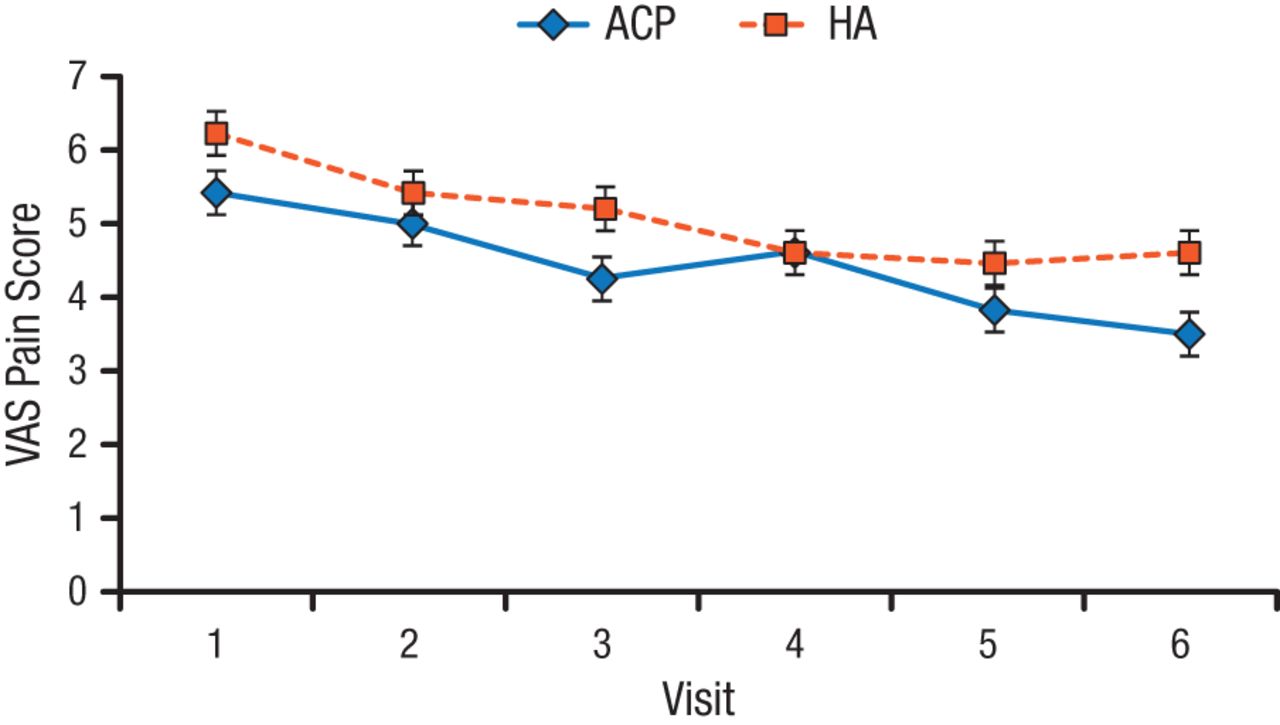
Lower VAS Pain Score With PRP vs HA
ACP, autologous conditioned plasma; HA, hyaluronic acid; PRP, platelet-rich plasma; VAS, visual analog scale.
Reproduced with permission from BJ Cole, MD.
Synovial analysis showed significantly higher interleukin-6 concentrations in PRP-treated patients compared with HA-treated patients at 6 months (P = .02), but no differences between the cohorts was seen in other catabolic factors analyzed.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.