

Summary
In patients with moderate to severe lumbar spinal stenosis and back pain, use of an interlaminar stabilization device after surgical decompression achieves significantly superior clinical outcomes at 3-year follow-up compared with use of standard treatment with posterolateral fusion, suggesting increasingly favorable clinical and radiographic outcomes with ILS compared with fusion in these patients.
- lumbar spinal stenosis
- interlaminar stabilization device
- posterolateral fusion
- spine conditions
- orthopaedics & sports medicine clinical trials
- orthopaedic procedures
Use of an interlaminar stabilization device (ILS) after surgical decompression in patients with moderate to severe lumbar spinal stenosis (LSS) and axial back pain with or without spondylolisthesis achieves significantly superior clinical outcomes at 3-year follow-up compared with use of standard treatment with posterolateral fusion.
Although fusion after decompression can provide relief from symptoms in the short term, recurring pain, pseudarthrosis, or degeneration at the adjacent levels may occur over the longer term. To evaluate and compare longer-term outcomes between the use of posterolateral fusion or ILS after decompression for LSS with back pain, Christopher A. Yeung, MD, Desert Institute for Spine Care, Phoenix, Arizona, USA, and colleagues conducted a prospective, randomized clinical trial that included 322 patients with moderate to severe LSS treated with either ILS (n = 215) or fusion (n = 107) after decompression.
Patients were recruited from 21 sites in the United States under a FDA investigational device exemption. All patients in the study had LSS at 1 or 2 contiguous levels between L1 and L5 confirmed on magnetic resonance imaging, as well as a visual analog scale back score of ≥ 50 mm.
The primary clinical outcome of the study was a composite clinical success rate that included achieving ≥ 15-point improvement (out of 100) on the Oswestry Disability Index (ODI) at 24 months, no reoperations, and no use of lumbar steroid injections. This 3-year follow-up study was part of the FDA’s postapproval requirement. Of the 322 patients in the study, 90.7% of the ILS group and 87.7% of the fusion group were available at 3-year follow-up.
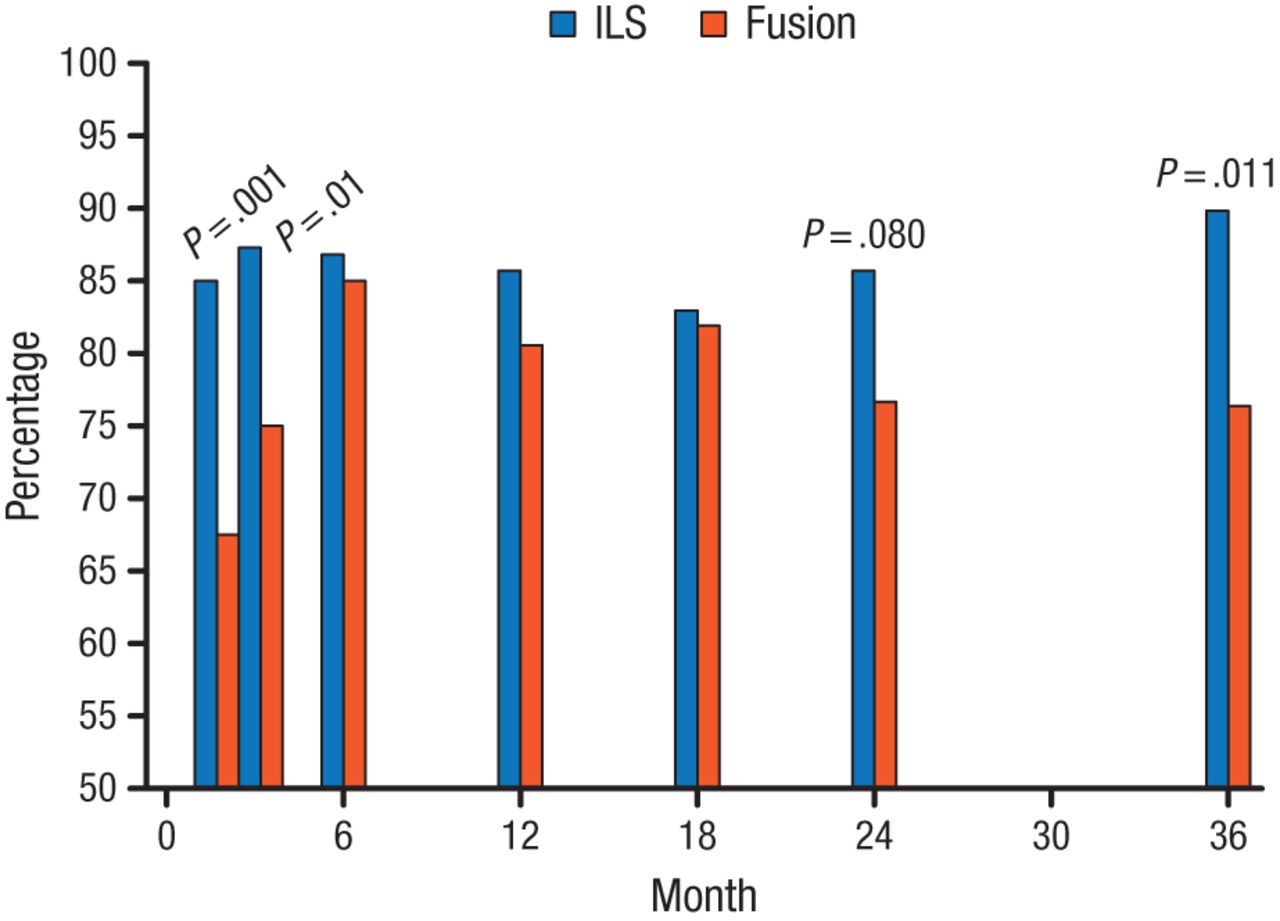
At year 3, the study found that significantly more patients treated with ILS achieved composite clinical success compared with the fusion group (62.8% vs 47.4%; P > .016). When broken down by individual clinical outcomes, the reoperation/injection rate at 3 years was 25% and 24% for ILS and fusion patients, respectively. Among the patients who did not require reoperation or injection, those treated with ILS had significant improvement in ODI compared with those treated by fusion (90% vs 79%; P = .011; Figure 1).
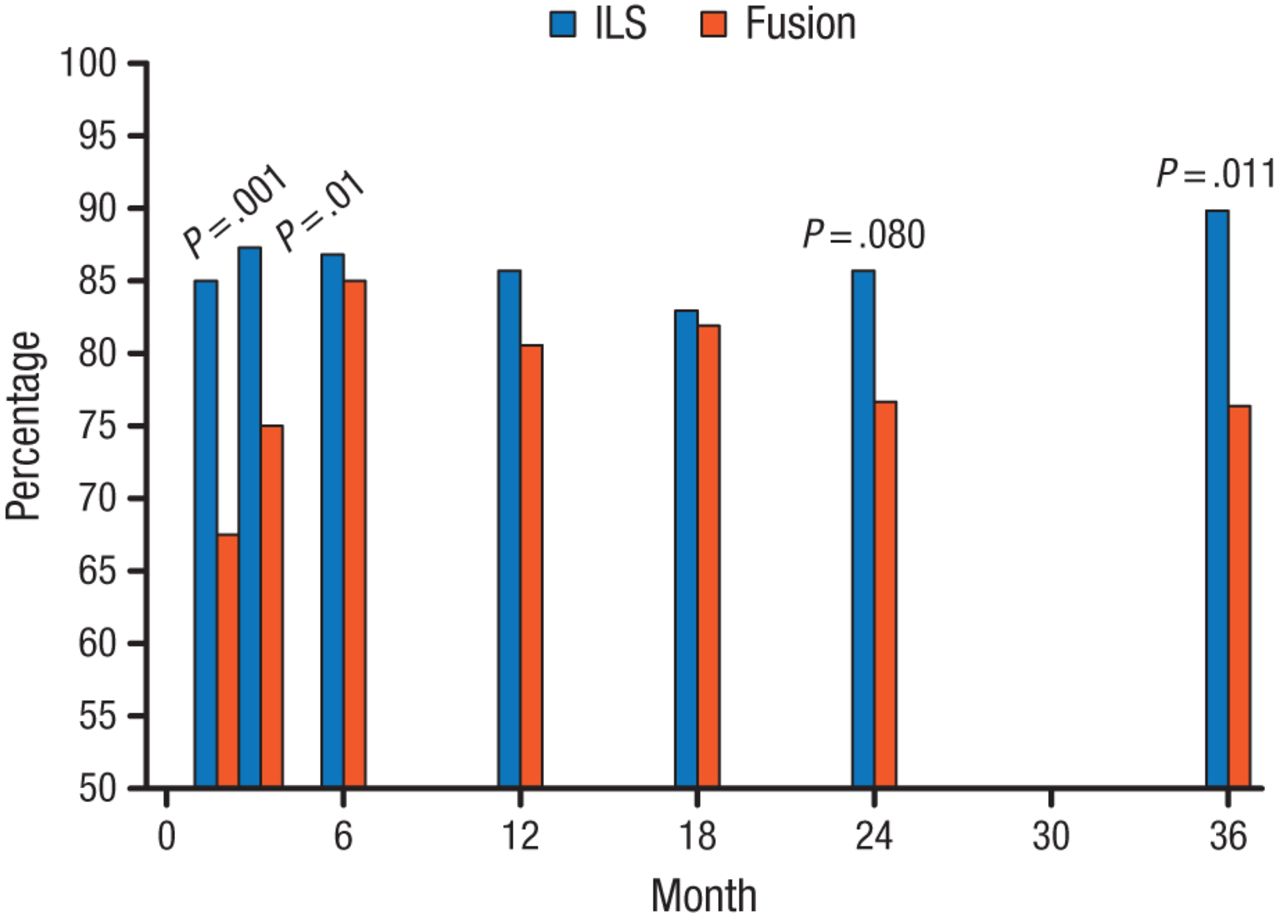
Percentage of Patients With ≥ 15-Point Improvement in Oswestry Disability Index
ILS, interlaminar stabilization device.
Reproduced with permission from CA Yeung, MD.
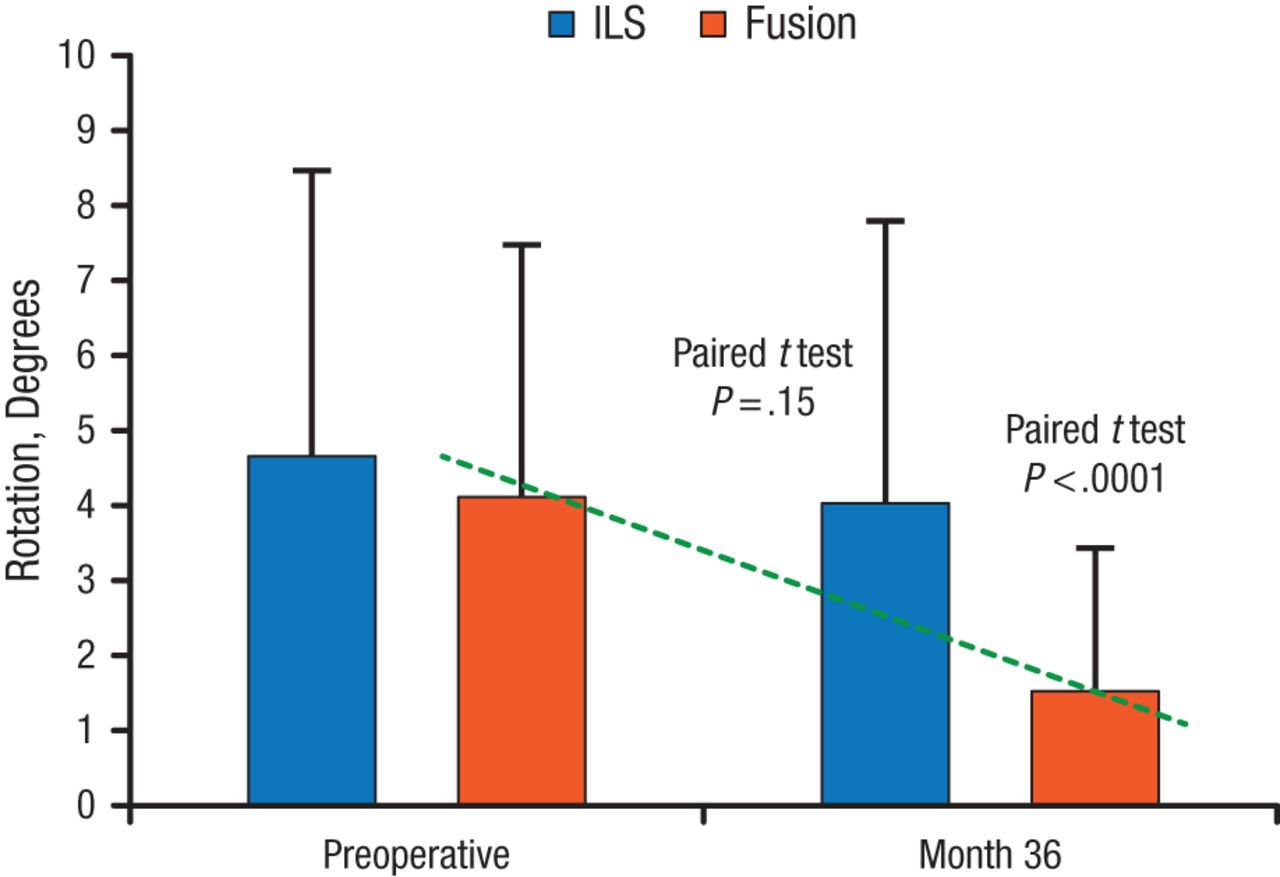
When looking at radiographic change between the 2 cohorts, the study found no significant implant-level radiographic change in motion as measured by flexion/extension radiographs in the ILS cohort (mean change at 3 years, –0.44°; P = .14), but a significant reduction in motion at the implant level in the fusion cohort (mean change at 3 years, –2.75°; P < .0001). The difference in radiographic change at 3 years between the 2 groups was significant (P < .0001; Figure 2).
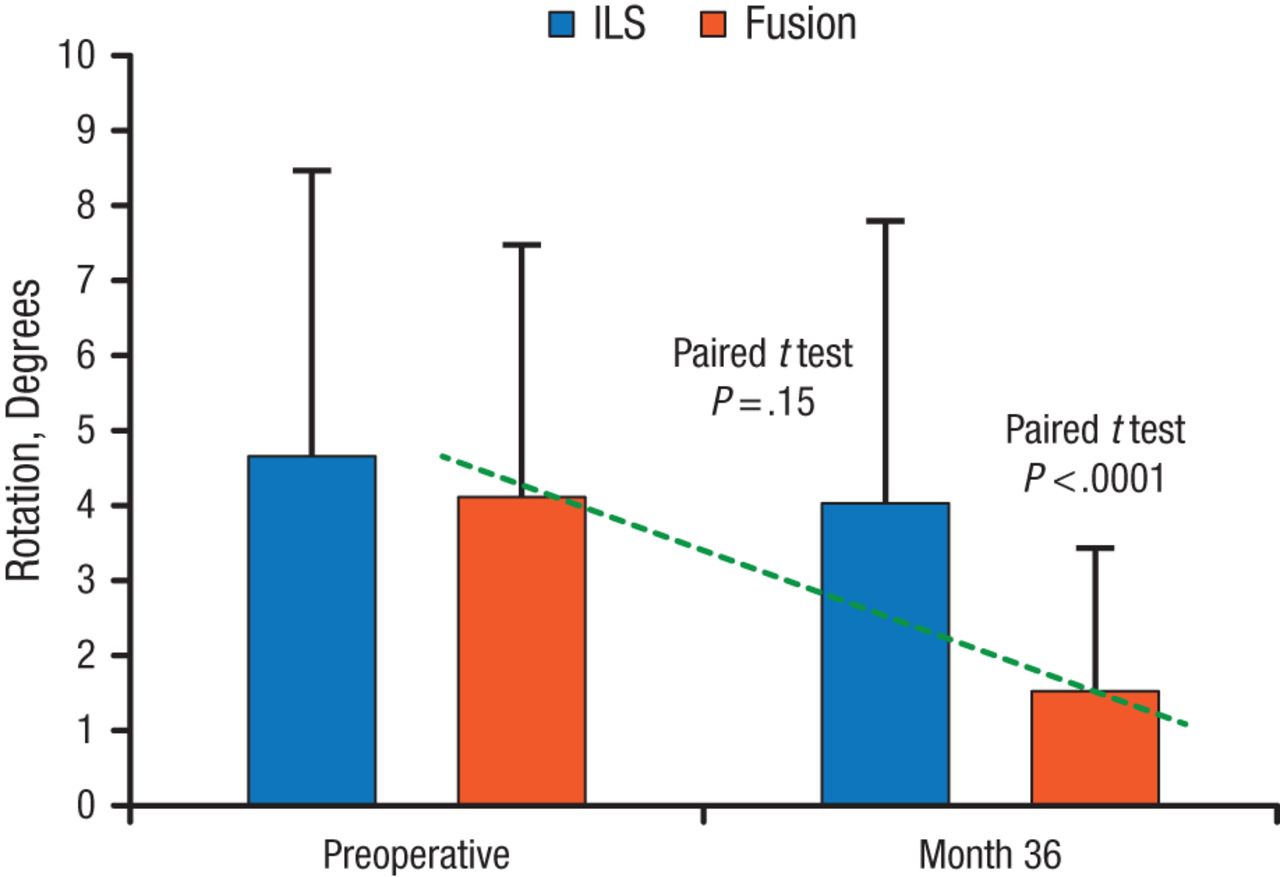
Mean (SD) Rotation at Baseline and Year 3
ILS, interlaminar stabilization device.
Reproduced with permission from CA Yeung, MD.
Radiographic analysis at 3 years shows adjacent level motion remains at preoperative levels in patients treated with ILS compared with significantly elevated adjacent level motion in patients treated by fusion. When looking only at the ILS group, the study also found that foraminal heights remained stable from preoperative to 3-year measurements (17.72 and 17.39 mm, respectively). Overall, these longer-term data suggest increasingly favorable clinical and radiographic outcomes with ILS compared with fusion in patients with moderate to severe LSS and back pain.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.