

Summary
The new American Heart Association/American College of Cardiology valvular heart disease guideline outlines approaches for quantification of valvular disease severity. Stage identification is key to determining severity, intervention, and prognosis. Surgical management is expanded to a subset of asymptomatic severe aortic stenosis, and transcatheter aortic valve replacement is increasingly recommended for higher-risk patients.
- aortic stenosis
- AHA/ACC valvular heart disease guideline
- mitral regurgitation
- tricuspid regurgitation
- staging of AS
- Doppler echocardiography
- dobutamine stress echo test
- aortic valve replacement
- imaging modalities
- cardiology & cardiovascular medicine guidelines
A panel of experts reviewed recommendations and insights for echo grading of aortic stenosis (AS), differentiating primary and secondary mitral regurgitation (MR), and quantifying changes in valvular structure and the severity of tricuspid regurgitation from the 2014 American Heart Association/American College of Cardiology (AHA/ACC) guideline for the management of patients with valvular heart disease [Nishimura RA et al. J Thorac Cardiovasc Surg. 2014; Circulation. 2014; J Am Coll Cardiol. 2014].
The 10 most important new concepts introduced in the 2014 valvular heart disease guideline, reviewed by James D. Thomas, MD, Northwestern University, Chicago, Illinois, USA, are summarized in Table 1.
Ten Key Messages From the 2014 AHA/ACC Valvular Heart Disease Guideline
Philippe Pibarot, DVM, PhD, Quebec Heart and Lung Institute, Montreal, Quebec, Canada, discussed echo grading of AS (Table 2). He noted that in low-flow states, it is difficult to distinguish true- from pseudo-severe AS. The AHA/ACC 2014 guideline recommends a dobutamine stress echo to detect contractile reserve. By augmenting stroke volume by ≥ 20%, the mean gradient should increase while the aortic valve area (AVA) remains severe (ie, ≤ 1.0 cm2) in true-severe AS. For patients without evidence of contractile reserve, a high aortic valve calcium score by multiple-detector computed tomography (CT) is able to different true- from pseudo-severe AS. Aortic valve replacement (AVR) is recommended for symptomatic patients with a gradient increase ≥ 40 mm Hg and an AVA ≤ 1.0 cm2 at any dobutamine dose (class IIa, level B).
Echo-Determined Staging of Symptomatic Severe AS
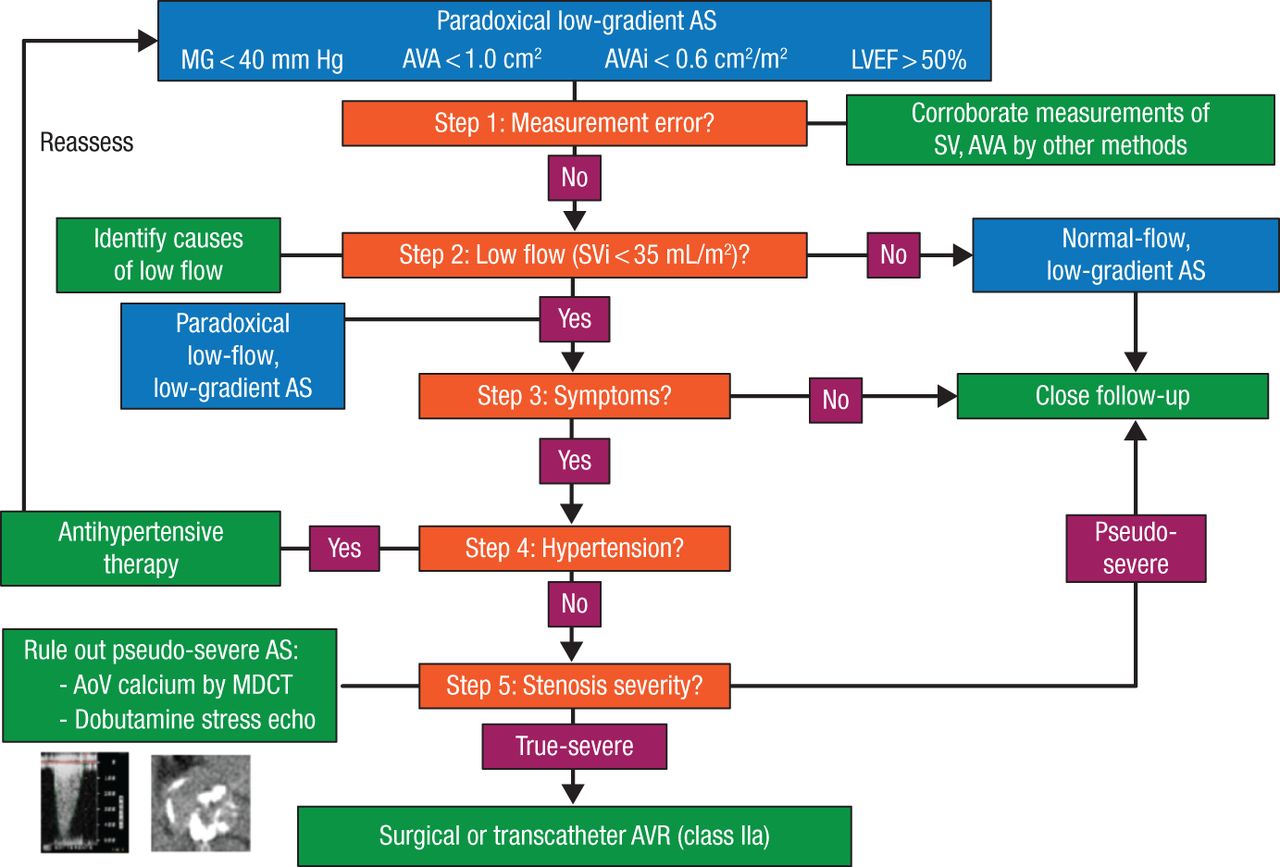
Paradoxical low-flow, low-gradient AS with preserved left ventricular (LV) ejection fraction is more often seen in elderly women with comorbid hypertension, metabolic syndrome, diabetes mellitus, and diastolic dysfunction, noted Prof Pibarot. AVR is reasonable in these patients if they are normotensive and if severe valve obstruction is the most likely cause of the symptoms (class IIa, level C). Aortic valve calcium scoring by multislice CT may be used to confirm stenosis severity in patients with paradoxical low-flow, low-gradient AS. However, different cut points of aortic valve calcium score should be used in women (> 1200 AU) vs men (2000 AU) to identify true-severe AS. The flow chart in Figure 1 provides an organized way to determine the appropriate treatment path for the patient.
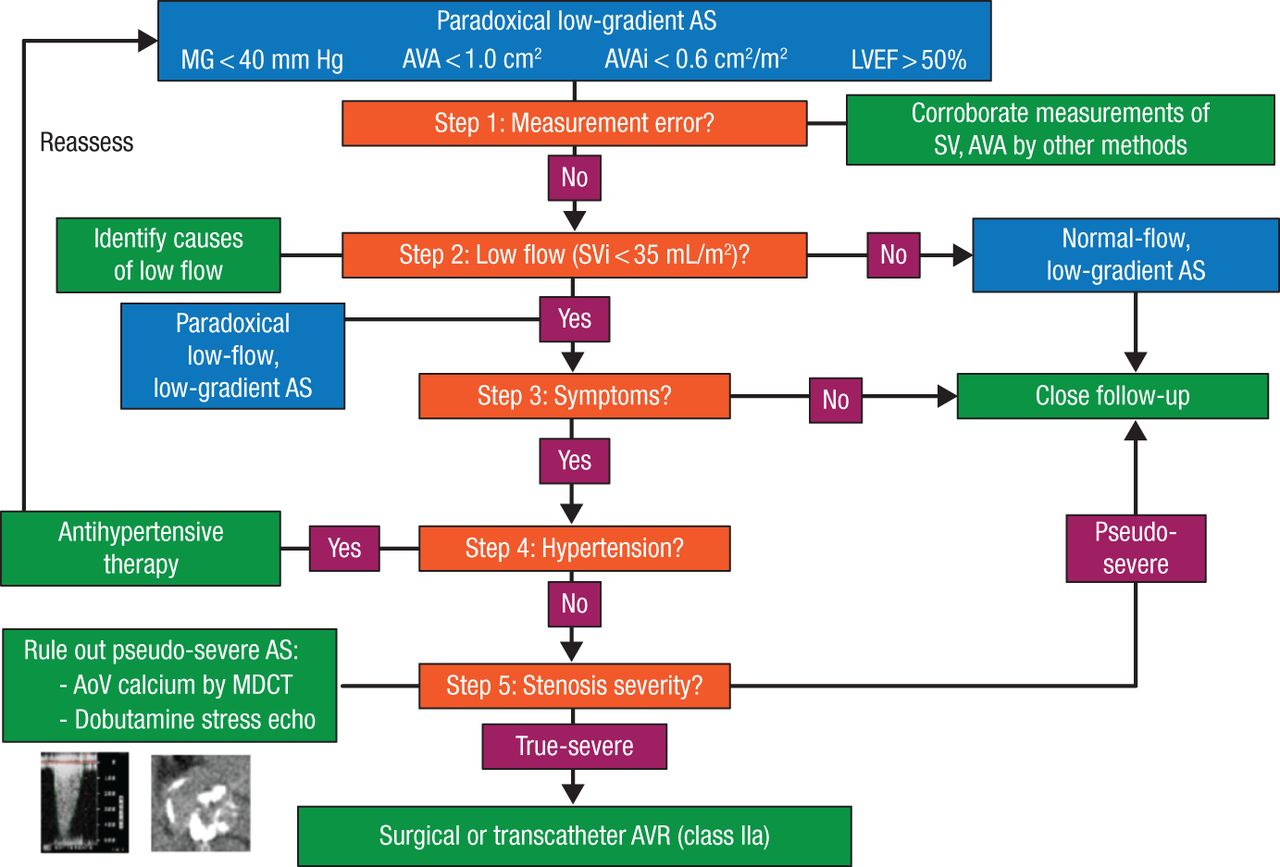
Decision Making in “Paradoxical” Low-Gradient AS
AoV, aortic valve; AS, aortic stenosis; AVA, aortic valve area; AVAi, aortic valve area index; AVR, aortic valve replacement; LVEF, left ventricular ejection fraction; MDCT, multidetector computed tomography; MG, mean gradient; SV, stroke volume; SVi, stroke volume index.
Reproduced with permission from P Pibarot, DVM, PhD.
Paul A. Grayburn, MD, Baylor Scott & White Health, Dallas, Texas, USA, outlined the differences between primary (degenerative) and secondary (functional) MR as reviewed in the AHA/ACC 2014 guideline. In primary MR, the leaflets are abnormal (eg, mitral valve prolapse), and surgical valve repair is the standard. The more difficult secondary MR has normal-appearing leaflets and is caused by LV dilation/dysfunction. Surgery has a class IIb recommendation (except during coronary artery bypass graft), as it is not clear if MR repair provides any benefit.
Secondary MR often results from LV dysfunction and/or remodeling due to either ischemic or nonischemic cardiomyopathy. These patients can also have a relatively preserved LV but significant MR due to an inferoposterior myocardial infarction or pure annular dilation. Clinically, they resemble patients with primary MR and may benefit from intervention targeted to the pathology. Dr Grayburn recommended careful use of specific echo measurements to determine the mechanism of MR (eg, leaflet tenting area, tethering distance, and annulus shape), as well as quantification of MR severity before making a management decision.
Linda D. Gillam, MD, Morristown Medical Center, Morristown, New Jersey, USA, discussed the AHA/ACC 2014 guideline options for assessment of aortic and pulmonic regurgitation. Echocardiography with Doppler is recommended as the primary means for noninvasive evaluation of native valvular regurgitation [Lancellotti P et al. Eur J Echocardiogr. 2010]. Two-dimensional echocardiography with color flow and spectral Doppler provides an assessment of valvular structure, mechanism of regurgitation, and adaptation to the volume overloaded state [Skaug TR. Eur Heart J Cardiovasc Imaging. 2014].
Echocardiographic quantification of aortic regurgitation can be best estimated using a variety of techniques, including color flow jet width, vena contracta width, proximal isovelocity surface area, descending aortic flow reversal, and quantification of regurgitant volume and fraction. In addition, assessment of the valve anatomy, etiology of dysfunction, and cardiac chambers is used in the management of valvular regurgitation and timing of surgery. In the future, real-time 3D imaging will provide enhanced measurements of flow convergence, vena contracta, and the regurgitant jet for improved quantitation of valvular regurgitation. The assessment of pulmonary regurgitation has much less validated methodology. Assessment of the valve morphology (typically congenital disease or iatrogenic), color flow analysis, and measurement of right ventricle size and function are most helpful. Dr Gillam reminded the audience to be aware of severe low-pressure pulmonary regurgitation, which can have laminar flow and thus sometimes be missed.
Lawrence Rudski, MD, McGill University, Montreal, Quebec, Canada, discussed AHA/ACC guideline methods to quantify the severity of tricuspid regurgitation, which may lead to right-sided failure with clinical implications, such as peritoneal and lower extremity edema, gut congestion, atrial fibrillation, and possibly increased risk of death.
Although there are limitations, the simplest and quickest way to measure tricuspid regurgitation severity is with color Doppler. The larger the color jet, the more significant the tricuspid regurgitation. This works well for mild or very severe tricuspid regurgitation, but when the degree of tricuspid regurgitation is uncertain, quantitation is mandatory. Proximal isovelocity surface area and derived effective orifice area, as well as vena contracta, are commonly employed quantitative methods and use color. Hepatic vein systolic flow reversal, triangulation and increased density of the tricuspid regurgitation signal, and increased right atrial and ventricular size are also useful tools for comprehensive, noninvasive quantitation of tricuspid regurgitation. Echo remains the most commonly used standard tool for assessment, but magnetic resonance imaging is still useful in some situations to quantify the impact of tricuspid regurgitation on right ventricular volumes and function.
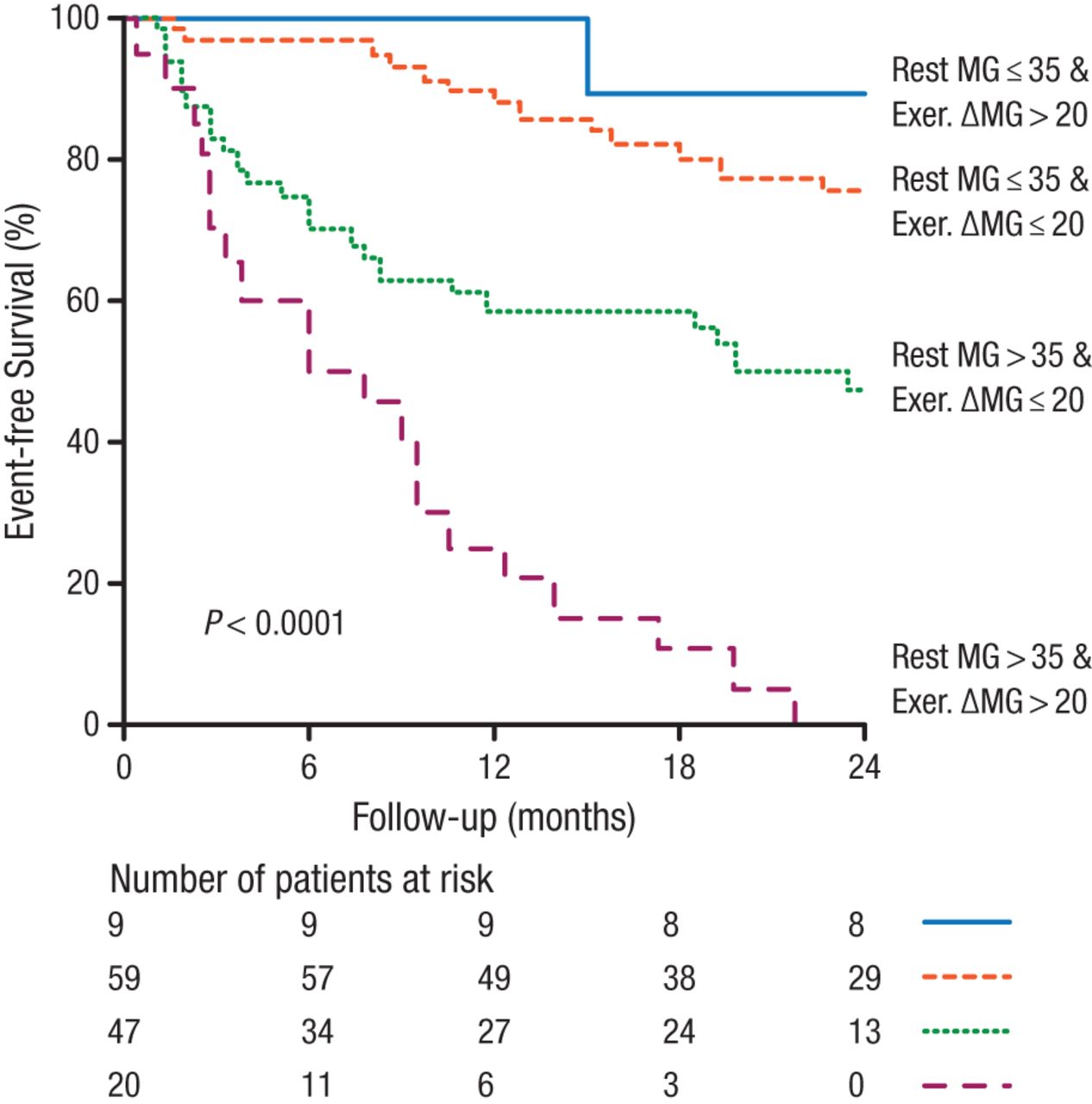
Paul Sorajja, MD, Minneapolis Heart Institute, Abbot Northwestern Hospital, Minneapolis, Minnesota, USA, addressed assessment of the functional severity of asymptomatic AS with stress testing. The AHA/ACC 2014 guideline recommends exercise stress testing for asymptomatic patients to assess physiologic changes and whether symptoms can be precipitated (class IIa). A “positive” test is one with symptoms, an ischemic echocardiogram, or a blood pressure reduction and is associated with a poor prognosis unless AVR is performed (class IIa). One study has shown that exercise-induced increases in the transaortic gradient add incremental prognostic value in AS patients with a normal exercise response (Figure 2) [Maréchaux S et al. Eur Heart J. 2010].
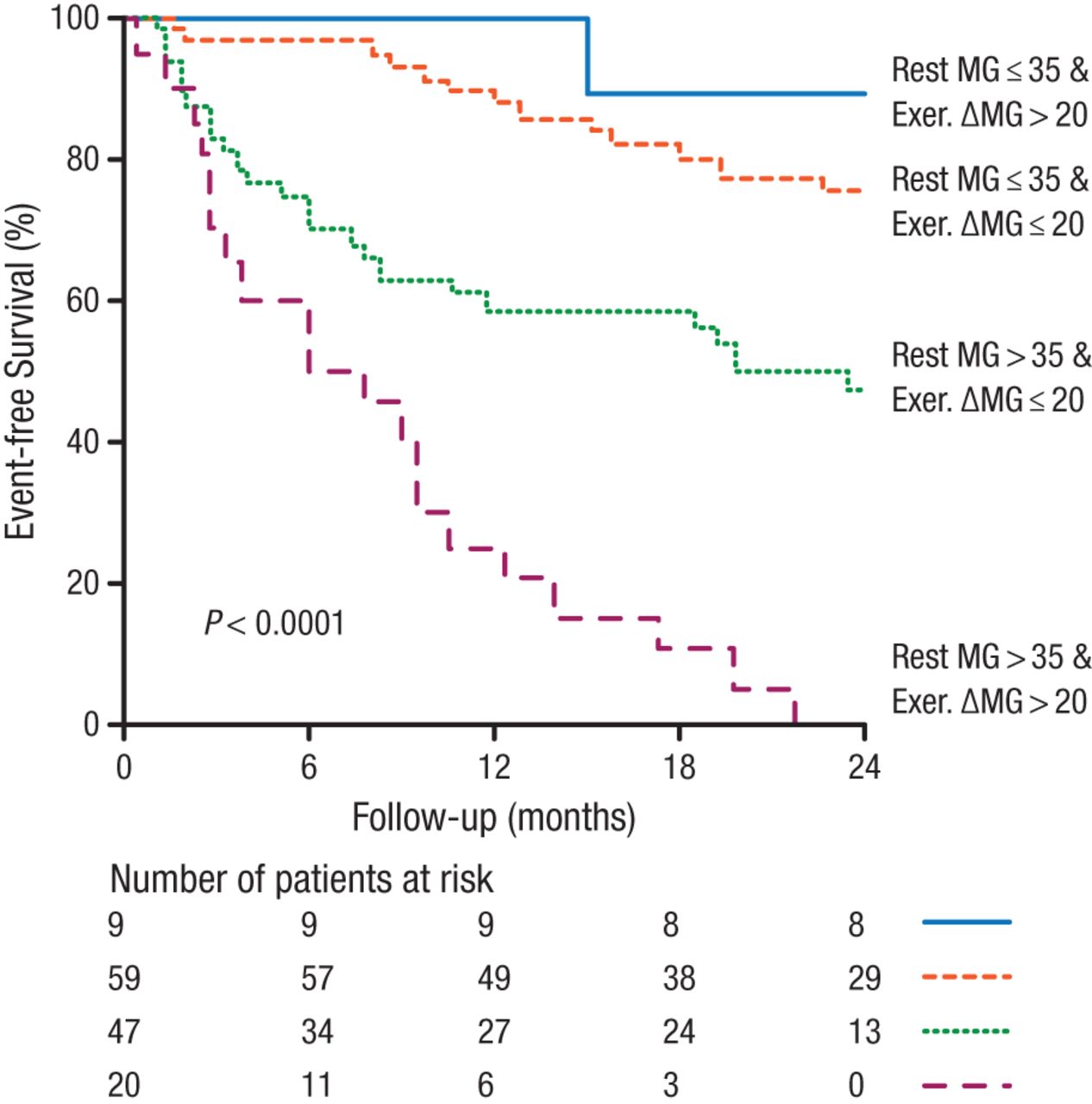
Significance of Exercise Gradient
MG, mean gradient.
Marechaux S et al. Usefulness of exercise-stress echocardiography for risk stratification of true asymptomatic patients with aortic valve stenosis. Eur Heart J. 2010;31(11):1390-1397. By permission of European Society of Cardiology.
Exercise testing is also recommended to evaluate the gradient and pulmonary artery systolic pressure in mitral stenosis where there is a discrepancy between the rest echo findings and the clinical symptoms or signs. The AHA/ACC 2014 guideline also states that exercise testing is reasonable for similar discrepancies with chronic primary MR (class IIa) or to establish symptom status (class IIa). For both mitral stenosis and regurgitation, exercise testing is useful for identification of those patients at higher risk of adverse clinical outcomes.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.