

Summary
This article highlights the serious global issue of stroke health disparities and discusses strategies to help reduce the problem. These include approaches focusing on health equity, health equity supplemented with targeted treatment, community-based participatory research, and involvement of other groups with an interest in reducing the disparity.
- stroke
- stroke disparities
- health equity
- targeted treatment
- community-based participatory research
- patient advocacy
Lewis B. Morgenstern, MD, University of Michigan, Ann Arbor, Michigan, USA, discussed approaches to address the international problem of stroke health disparities in the William M. Feinberg Memorial Lecture.
According to Dr Morgenstern, stroke disparities can be defined as the increased stroke incidence or worse associated outcomes that are correlated with factors such as race, ethnic origin, sex, socioeconomic status, or geographic location. In his discussion on the evidence that demonstrates the consequences of treatment inequities on disease outcomes [Smedley B. Am J Public Health. 2012], he highlighted the critical need to remedy this issue and proposed 2 potential approaches.
Health Equity
The health equity approach involves treating all patients equally, said Dr Morgenstern, and, in his opinion, should be mandatory. One advantage to this approach is its moral fairness; it does not single out individuals based on race, ethnic origin, or socioeconomic status.
Recent data from the South London Stroke Register discussed the effect of socioeconomic deprivation on stroke health care in England [Chen R et al. J Neurol Neurosurg Psychiatry. 2014]. The data showed that stroke health care inequalities exist and that, in particular, the impact of socioeconomic deprivation may be increased in black patients compared with white patients. Although the issue of stroke health care inequality in England has somewhat improved over time, there is need for further improvement.
Dr Morgenstern also shared the results of a recent study on quality and equity of care in hospitals in the United States [Trivedi AN et al. N Engl J Med. 2014]. The study compared between- and within-hospital differences between black and white patients from 2005 to 2010 for percutaneous coronary intervention, pneumococcal vaccination, and influenza vaccination. Data showed marked reductions in both the between- and within-hospital differences for these important quality measures. In a comparison of non-Hispanic white and Hispanic patients, the differences for the same quality measures, as well as for smoking cessation, were almost reversed during that period, indicating that improvement efforts to promote health equality are making a significant difference.
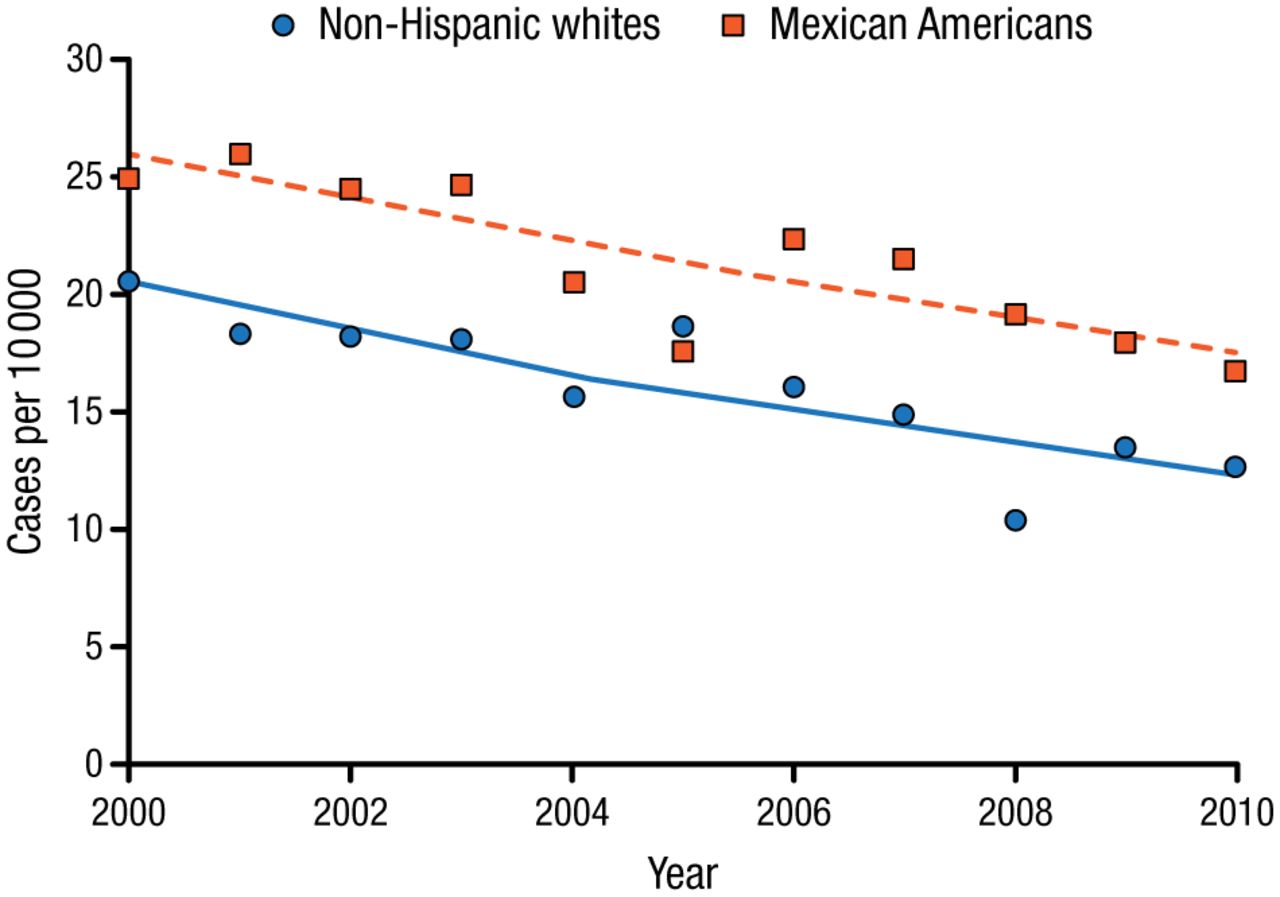
However, Dr Morgenstern noted that one disadvantage of this health equity approach lies in its assumption that disparities are due only to bias or discrimination. To underline this point, he shared data from another 10-year study comparing the incidence of stroke in Mexican Americans and non-Hispanic whites [Morgenstern LB et al. Ann Neurol. 2013]. While the study demonstrated a marked reduction in stroke incidence over the 10-year period, the disparity remained unchanged, with Mexican Americans having an increased stroke incidence compared with non-Hispanic whites (Figure 1).
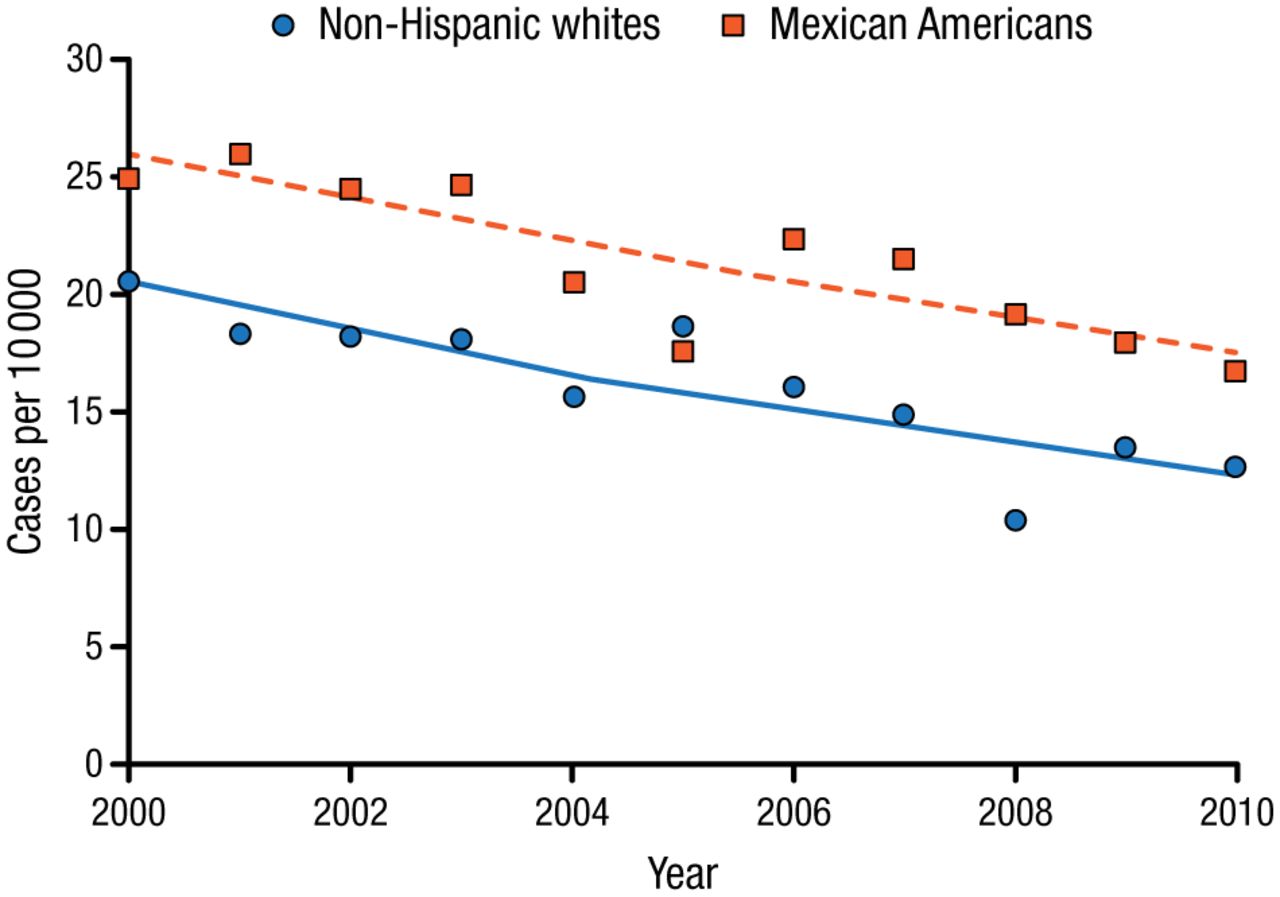
Incidence of Stroke in Mexican Americans and Non-Hispanic Whites (2000-2010)
Adapted from Morgenstern LB et al. Persistent ischemic stroke disparities despite declining incidence in Mexican Americans. Ann Neurol. 2013;74:778-785. With permission from American Neurological Association.
Giving a second example of this phenomenon, Dr Morgenstern discussed findings that were reported following another recent study comparing low-density lipoprotein cholesterol (LDL-C) control in black and white patients with diabetes from 2008 to 2010 [Zhang R et al. Am J Med Qual. 2013]. At baseline, LDL-C control was demonstrated in 55% of white patients and 49.8% of black patients. Paradoxically, however, even after a physician-directed quality improvement initiative was employed in an attempt to improve LDL-C control, the disparity increased, with 61.8% of whites and 44.6% of blacks having LDL-C control in 2010. These findings clearly suggest that, although health equality is critical to the process of improving health disparities, it may not be enough on its own to completely eliminate them.
Health Equity Combined with Targeted Treatment
Consequently, according to Dr Morgenstern, a second approach for prevention and preparedness involves targeting highest-risk populations, in combination with the health equity approach.
This approach requires the consideration of other factors, including the following:
-
Access to health care and insurance status
-
Behavioral risk factors (eg, diet and exercise)
-
Biological risk factors (eg, genetics)
It also acknowledges the key issues of continued residential segregation and the increasing income gap between the rich and poor that prevents many people from being able to live in safe neighborhoods and access good food and quality health care.
Dr Morgenstern shared data from a study aimed at a low-socioeconomic-status population, demonstrating a 2.5-fold increase in quit rate in those who were randomized to enter a smoking intervention program as compared with those in the control group (OR, 2.5; 95% CI, 1.5 to 4.0; P < .001) [Haas JS et al. JAMA Intern Med. 2014].
He also presented results from a Nigerian treatment adherence trial in which 544 patients with previously untreated hypertension were randomized to a nurse-led clinic visit or a clinic and a home visit [Adeyemo A et al. J Hypertens. 2013]. All patients received relatively inexpensive antihypertensive drugs. Three-fourths of participants completed the 6-month study, with almost complete treatment compliance (98%) that resulted in blood pressure (BP) control in two-thirds of participants.
In another international study, participants in China and Nigeria were randomized to a cardiovascular intervention comprising education and low-cost antihypertensive drugs vs control [Mendis S et al. Bull World Health Organ. 2010]. At the end of the study, patients in the intervention group had lower BP. Although half the participants in the intervention group still had uncontrolled BP, Dr Morgenstern acknowledged that reductions in BP of 13 and 11 mm Hg in China and Nigeria, respectively, are substantial and important in reducing stroke risk in these populations. Also, because BP reduction was observed in the control group, he suggested that performing clinical trials for stroke prevention in the developing world might even be beneficial in and of itself.
However, Dr Morgenstern did note that this combined approach can be expensive and may lead some to question why certain groups receive resources while others do not. He also emphasized that this approach of targeting individuals “for their own good” is viewed as condescending by others and is not what everyone wants.
He therefore discussed some additional strategies that have been used to help address health disparities. Community-based participatory research is one alternative that focuses on research that is important to the community, and it involves community members and researchers forming a true partnership to help conduct, implement, and sustain the research [Skolarus LE et al. Stroke. 2011]. Another strategy involves integrating others with an interest in reducing health disparities, such as large employers. Dr Morgenstern discussed one study that showed how disparities in cardiovascular disease create a significant financial incentive for employers and insurers to improve the health of minority groups, decrease costs, and reduce disparities [Burke JF et al. Am J Manag Care. 2014].
In his final remarks, Dr Morgenstern urged physicians to be active in reducing and eliminating health disparities. Emphasizing ways in which physicians can make a difference, he suggested that they devote 5% of their work time to research, clinical, or advocacy issues that directly benefit poor and underserved populations and reduce disparities. By advocating for patients in this way, physicians will ultimately benefit the most, he concluded.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.