

Summary
An analysis of the MR CLEAN trial demonstrated a significant interaction between time from stroke onset to reperfusion and treatment effect, with the decrease in absolute risk difference between treated and untreated patients of almost 7% per hour (P = .038). The relationship between time to treatment and treatment effect was not statistically significant but is still considered biologically plausible.
- acute ischemic stroke
- endovascular
- intra-arterial
- MR CLEAN
- TOR
- TOT
Puck Fransen, MD, Erasmus MC University Medical Center, Rotterdam, The Netherlands, reported results of the analyses that examined the interaction between time from stroke onset to treatment (TOT) and time from stroke onset to reperfusion (TOR) and the effect of treatment on clinical outcome in the MR CLEAN trial, demonstrating that TOR significantly affected treatment outcome.
MR CLEAN was the first study to demonstrate efficacy of intra-arterial treatment received within 6 hours of stroke onset in patients with acute ischemic stroke due to intracranial anterior circulation occlusion [Berkhemer OA et al. N Engl J Med. 2015]. According to Dr Fransen, time is an important predictor of clinical outcome in all ischemic diseases, and this analysis was assigned to assess the interaction between TOT and TOR with treatment on clinical outcome and whether treatment was effective in the entire 6-hour time frame used in the trial.
The multicenter MR CLEAN was a randomized, prospective, open-label, phase 3 trial with blinded outcome assessment conducted in The Netherlands. The primary outcome measure in this analysis was the score on the modified Rankin Scale (mRS) at 90 days, with adjusted common odds ratio for shift on the mRS as the primary effect parameter.
The study enrolled a total of 500 patients (167 in early, 168 in medium, and 165 in late TOT groups). The main clinical characteristics—such as patient age, sex, and the National Institute of Health Stroke Scale score at baseline—were similar among the groups.
The median TOT (treatment defined as microcatheter in the groin) was 256 minutes, with 11.5% of patients receiving treatment in < 3 hours, 45% between 3 and 4.5 hours, 44% between 4.5 and 6 hours, and 8.8% in > 6 hours. The median TOR (reperfusion defined as achieving thrombolysis in cerebral infarction grade 2b/3—which has been regarded as a successful angiographic outcome—or end of the procedure if reperfusion was not reached) was 332 minutes, with 1.5% achieving reperfusion in < 3 hours, 22% between 3 and 4.5 hours, 40% between 4.5 and 6 hours, and 37% in > 6 hours.
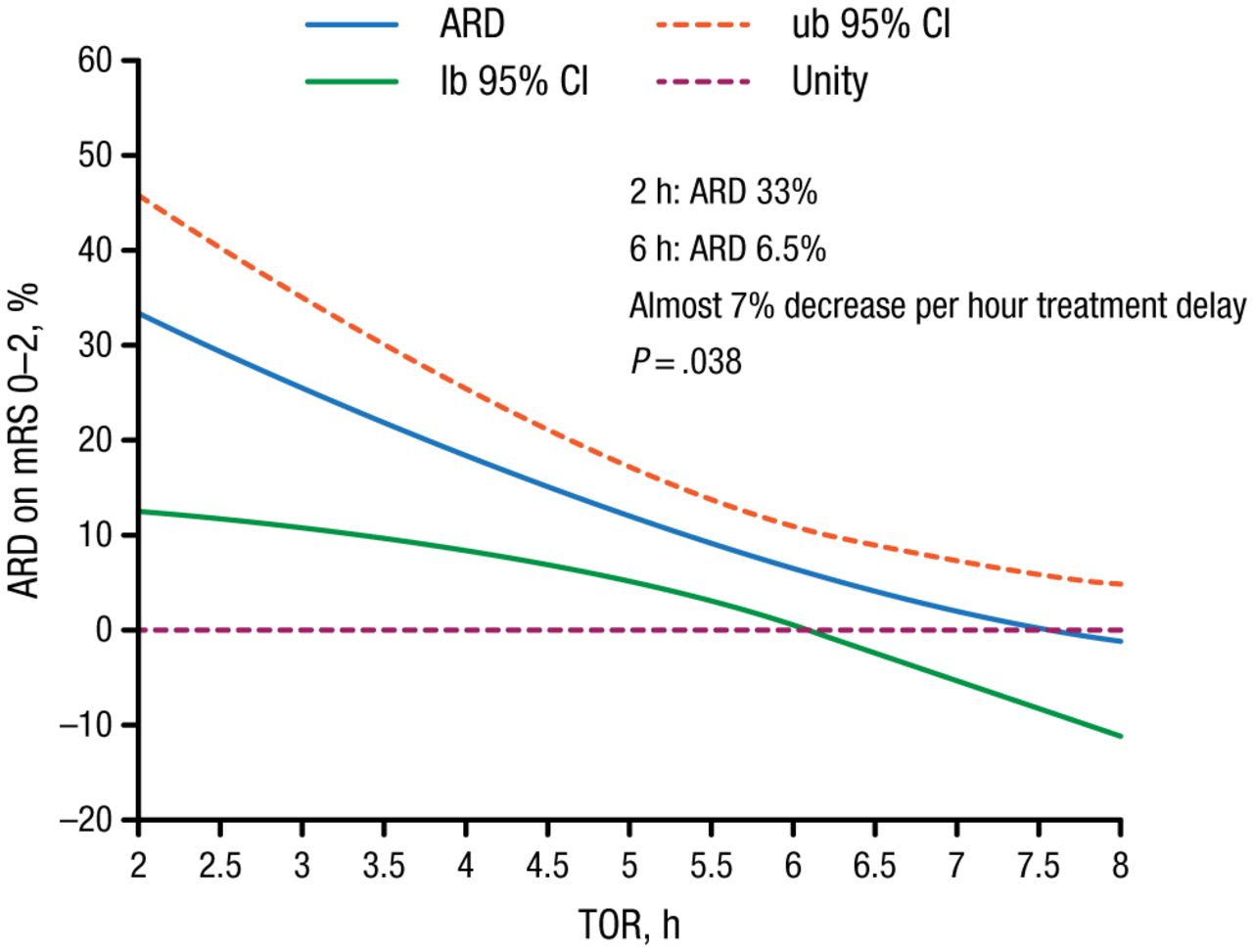
An analysis of the relationship between treatment effect and TOT suggested that the absolute risk difference (ARD) in chances of good outcome (mRS, 0-2) between treated and untreated patients was 19% at TOT equal to 2 hours and 3% at TOT equal to 6 hours. This implied a 4% decrease in ARD per hour, which was not statistically significant (P = .26). However, the decrease in ARD per hour of TOR was calculated to be almost 7% and statistically significant (P = .038), with ARD of 33% at 2 hours and 6.5% at 6 hours (Figure 1). The treatment effect was not statistically significant beyond TOR of 6 hours and 19 minutes.
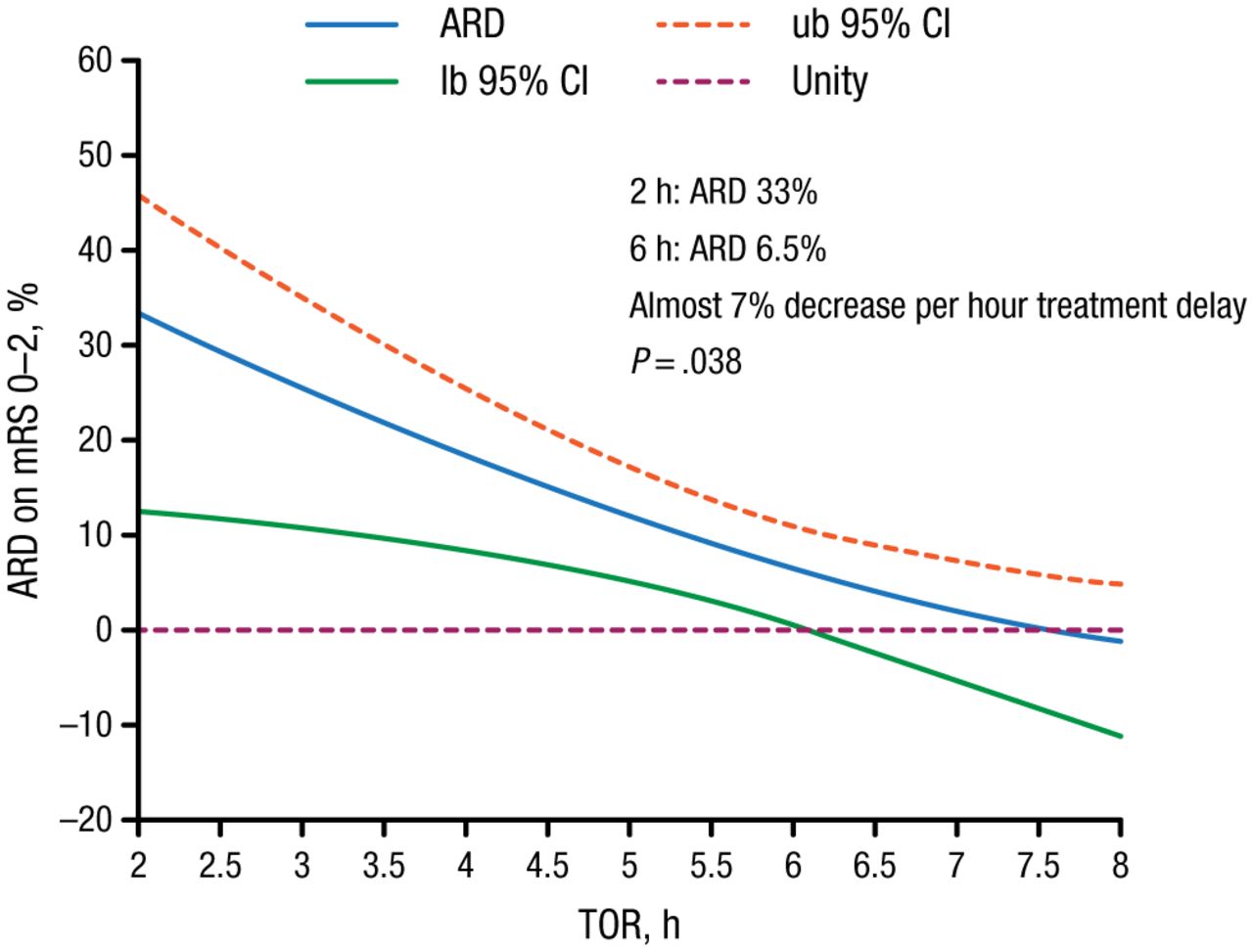
TOR Affects Chances of Good Outcome
ARD, absolute risk difference; lb, lower bound; mRS, modified Rankin Scale; TOR, time from stroke onset to reperfusion; ub, upper bound.
Reproduced with permission from P Fransen, MD.
Dr Fransen concluded that there was a significant interaction between TOR and treatment effect, while the interaction between TOT and treatment effect was not statistically significant but is still considered to be biologically possible. The study demonstrated that the probability of a positive outcome decreases rapidly with every hour of reperfusion delay, and patients with acute ischemic stroke should receive appropriate treatment as soon as possible.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.