

Summary
Although much has been written about the ill effects of high intake of dietary cholesterol and saturated fatty acids (SFAs) on cardiovascular disease (CVD), strong, consistent evidence for a beneficial effect from lowering dietary cholesterol and SFAs is limited. This article discusses where focus should be on eating healthy foods versus about SFAs and cholesterol intake.
- Lipid Disorders
- Nutrition Physiology
- Lipid Disorders
- Nutrition Physiology
- Nutrition
Although much has been written about the ill effects of high intake of dietary cholesterol and saturated fatty acids (SFAs) on cardiovascular disease (CVD), strong, consistent evidence for a beneficial effect from lowering dietary cholesterol and SFAs is limited. Ronald M. Krauss, MD, Children's Hospital Oakland Research Institute Oakland, California, USA, believes the focus should be on eating healthy foods and less about SFAs and cholesterol intake.
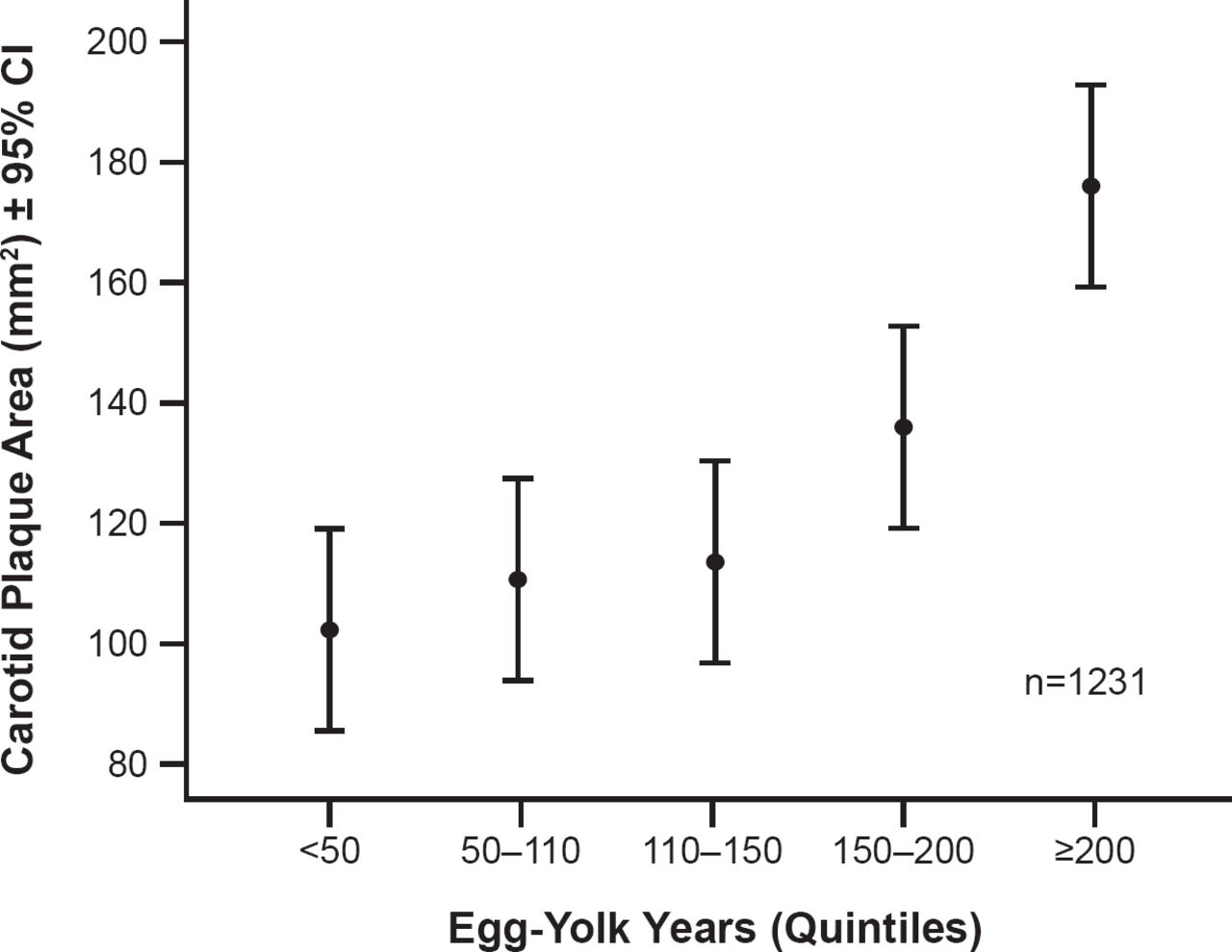
Evidence suggests that dietary cholesterol has small and variable effects on blood cholesterol in most persons; however, in some individuals these effects may be cause for concern. Results of a meta-analysis of 12 studies did not show a relationship between egg consumption and an increased risk of CVD and cardiac mortality in the general population. However, egg consumption may be associated with an increased incidence of type 2 diabetes and CVD comorbidity among diabetic patients [Shin JY et al. Am J Clin Nutr 2013]. Another recent study, however, reported an association between egg yolk consumption and carotid plaque in individuals at risk of CVD (Figure 1) [Spence JD et al. Atherosclerosis 2012].

Egg Yolk Consumption and Carotid Plaque
Reproduced from Spence JD et al. Egg yolk consumption and carotid plaque. Atherosclerosis 2012;224(2):469–473. With permission from Elsevier.
Another dietary concern is overconsumption of the SFAs that are found in animal-based foods such as dairy products and red meat, and coconut, palm, and palm kernel oils. SFAs raise levels of low-density lipoprotein (LDL) cholesterol, which is strongly linked to heart disease. The American Heart Association (AHA) recommends that individuals obtain <7% of their energy from SFAs [AHA Nutrition Committee et al. Circulation 2006]. In the United States, recent data indicate a small reduction in the percentage of calories consumed from SFAs as well as decreases in total serum cholesterol. However, the latter is attributed to an increase in the use of cholesterol-lowering medications rather than dietary changes [Ford ES, Capewell S. PloS One 2013].
LDL cholesterol is comprised of subclasses of particles with differing cholesterol content and CVD risk. SFAs appear to affect large LDL particles, which are less strongly associated with CVD. Carbohydrates have a major influence on smaller LDL particles, which have greater entry into the arterial wall and are subjected to faster oxidation. Moderate carbohydrate restriction can improve atherogenic dyslipidemia [Krauss RM et al. Am J Clin Nutr 2006].
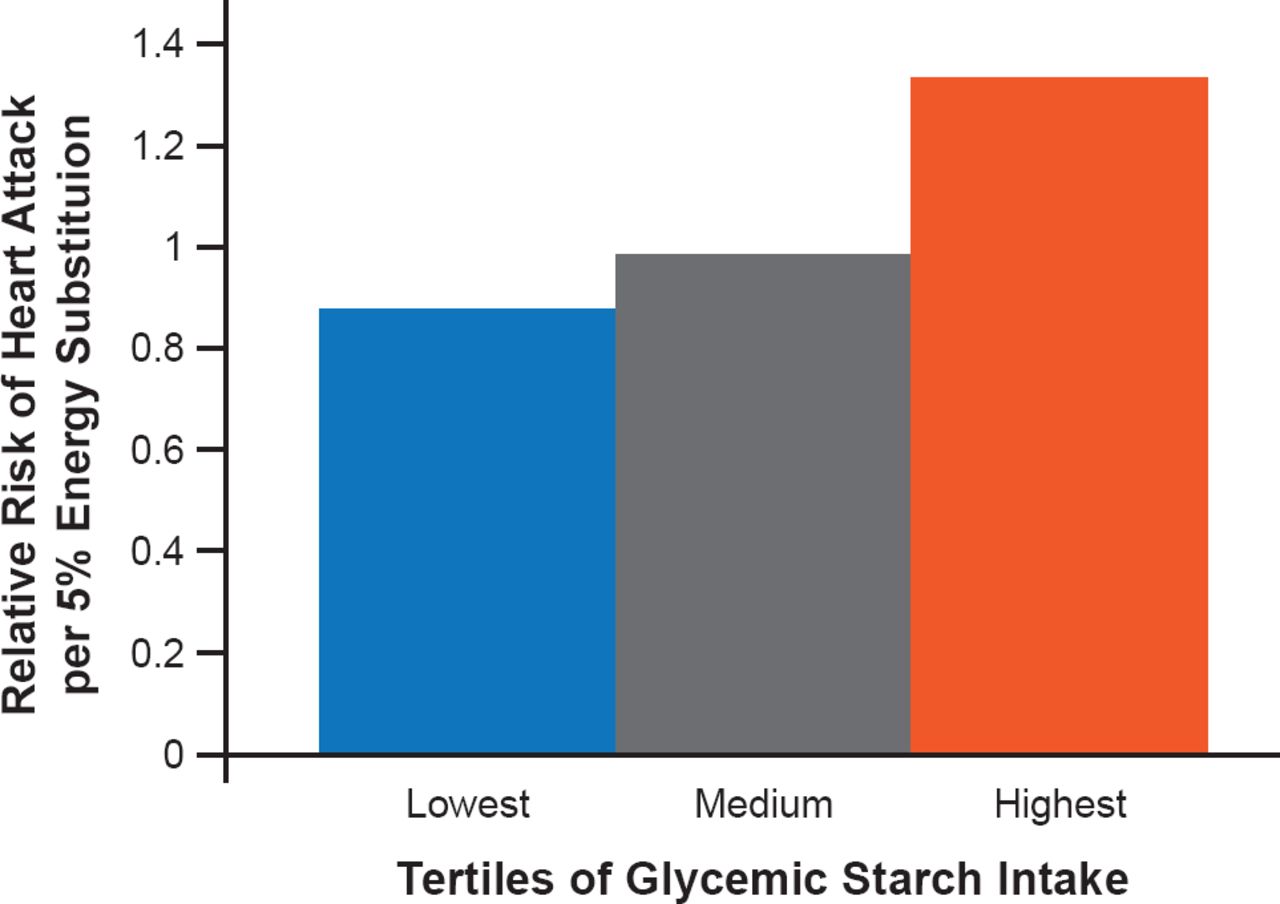
Epidemiologic evidence to date shows no reduction in heart disease when SFAs are replaced by carbohydrates, and there is some evidence that the risk may be increased. However, the type of carbohydrate may be important. In one study, replacing SFAs with carbohydrates with low-glycemic index values was associated with a lower risk of myocardial infarction (MI; HR, 0.88; 95% CI, 0.72 to 1.07), whereas replacing SFAs with carbohydrates with high glycemic index values was associated with a higher risk of MI (HR, 1.33; 95% CI, 1.08 to 1.64; Figure 2) [Jakobsen MU et al. Am J Clin Nutr 2010].

Risk of Heart Attack Increases as High Glycemic Index Carbohydrates Are Substituted for SFAs
Reproduced from Jacobsen MU et al. Intake of carbohydrates compared with intake of saturated fatty acids and risk of myocardial infarction: importance of the glycemic index. Am J Clin Nutr 2010;91(6):1764–1768. With permission from the American Society for Nutrition.
A meta-analysis of eight randomized controlled trials indicated that consuming polyunsaturated fatty acids (PUFAs) in place of SFA reduces coronary heart disease [Mozaffarian D et al. PLoS Med 2010]. Although challenged in a more recent meta-analysis [Ramsden CE et al. BMJ 2013], other evidence is strong that the risk of coronary heart disease is reduced when SFAs are replaced with PUFAs [Astrup A et al. Am J Clin Nutr 2011].
Low fat diets in general appear to be healthier. Among persons at high CV risk, a Mediterranean diet (fruits, vegetables, fish, and whole grains) supplemented with extra-virgin olive oil or nuts reduced the incidence of major CV events [Estruch R et al. N Engl J Med 2013].
Although studies of specific eating patterns such as the Dietary Approaches to Stop Hypertension (DASH) eating plan and the Mediterranean diet have shown CVD benefits, the actual beneficial element in the diet has not been conclusively identified. The evidence to date shows no clear benefit of substituting carbohydrates for SFAs although there might be a benefit if the carbohydrate is unrefined and has a low glycemic index [Astrup A et al. Am J Clin Nutr 2011]. The Women's Health Initiative trial, which assessed diets with reduced total fat intake and increased intakes of vegetables, fruits, and grains, showed no reduction of heart disease risk or stroke [Howard BV et al. JAMA 2006]. A meta-analysis of 21 prospective cohort trials supported these findings [Siri-Tarino PW et al. Am J Clin Nutr 2010].
It may be that the intake of red meat is responsible for much of the risk of heart disease (and diabetes) attributed to saturated fat. Red meat consumption has been associated with an increased risk of CVD and cancer mortality, while substitution of other healthy protein sources is associated with lower mortality risk [Pan A et al. Arch Intern Med 2012]. Elevated trimethylamine-N-oxide (a proatherosclerotic metabolite) levels, found in red meat predict an increased risk of major adverse CV events [Tang WH et al. N Engl J Med 2013].
Thus, it is not just the presence of cholesterol and saturated fat in the diet that matters; it is also the foods that are the sources of those factors. Individual SFAs may have different CV effects and major SFA food sources contain other constituents that could influence CVD risk. The combination of multiple biomarkers and the use of clinical endpoints could help substantiate the effects on CVD. In general, fatty fish, nuts, other polyphenol-rich foods, and legumes are good dietary choices, while trans-fats, sugars, and glycemic starches are not [Astrup A et al. Am J Clin Nutr 2011].
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.