

Summary
Bifurcation lesions occur at the point where one coronary artery branches from another. Currently, provisional side-branch stenting is the preferred strategy for treating most bifurcation lesions. This type of stenting involves stenting the main branch, reserving further stent placement in the side branch only if it is compromised. However, it is not known if provisional stenting provides the best outcomes in bifurcation lesions involving a large side branch. The aim of the Nordic-Baltic Bifurcation Study IV [NCT01496638] was to compare provisional stenting with a two-stent techniques for the treatment of true coronary bifurcation lesions involving a large side branch.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
- Interventional Techniques & Devices
Bifurcation lesions occur at the point where one coronary artery branches from another. Currently, provisional side-branch stenting is the preferred strategy for treating most bifurcation lesions. This type of stenting involves stenting the main branch, reserving further stent placement in the side branch only if it is compromised. However, it is not known if provisional stenting provides the best outcomes in bifurcation lesions involving a large side branch.
The aim of the Nordic-Baltic Bifurcation Study IV [NCT01496638], presented by Indulis Kumsars, MD, Pauls Stradins Clinical University Hospital, Riga, Latvia, was to compare provisional stenting with a two-stent techniques for the treatment of true coronary bifurcation lesions involving a large side branch. The study investigators hypothesized that a two-stent technique would be superior to provisional stenting in this setting.
This open-label trial randomized 450 patients with bifurcation lesions involving a large side branch to either provisional stenting (n=221) or a two-stent technique (n=229). Patients with bifurcation stenosis involving both the main vessel and the side branch were eligible. The patients could have stable angina, unstable angina, or non-ST-segment elevation myocardial infarction (NSTEMI), but were excluded if they had STEMI, cardiogenic shock, other critical illnesses, or if the side branch lesion was >15 mm long. The first 225 patients were treated with a sirolimus-eluting stent and the last 225 patients received an everolimus-eluting stent. The primary endpoint was major adverse cardiac events (MACE), defined as the composite of cardiac death, non-index procedure-related MI, target lesion revascularization, and definite stent thrombosis.
Baseline demographics and clinical characteristics were well balanced between the two groups. Lesion characteristics were similar between the provisional stent and two-stent groups, with the exception of the main vessel reference diameter (3.5 vs 3.4 mm; p=0.04) and the side branch lesion length (7.4 vs 8.0 mm; p<0.0001; Table 1).
Lesion Characteristics
Of the 450 randomized patients, 220 in the provisional stent group and 227 in the two-stent group were stented and completed 6 months of follow-up. The side branch was dilated in 64.3% of the provisional group and in 78.0% of the two-stent group. Final kissing balloon stent dilation was performed in 36.1% of the provisional group and in 91.2% of the two-stent group. Side branch stenting was performed in 3.7% of the provisional group and 96.0% of the two-stent group. When defining success as residual stenosis of <30% in the main vessel plus TIMI Grade III flow in the side branch, 97.7% of the provisional group and 99.1% of the two-stent group had successful procedures.
At 6 months, the primary endpoint of MACE had occurred in 4.6% of patients in the provisional stent group compared with 1.8% of patients in the two-stent group (p=0.09).
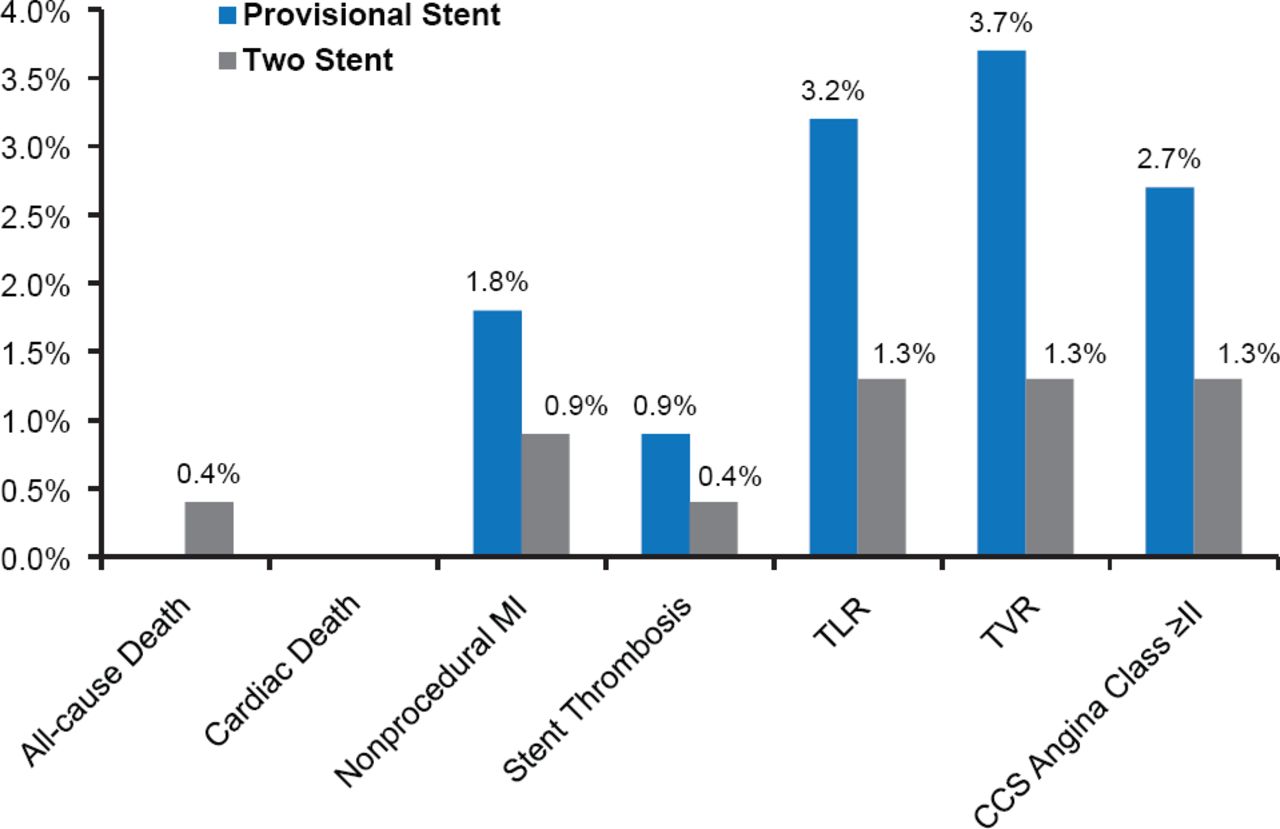
No differences between the provisional stent group and the two-stent group achieved statistical significance for the following secondary endpoints (Figure 1).

Secondary Endpoints
CCS=Canadian Cardiovascular Society; MI=myocardial infarction; TLR=target lesion revascularization; TVR=target vessel revascularization.
At 6 months, there were no statistically significant differences in the rate of MACE between patients treated with provisional stenting and those treated with a two-stent technique for bifurcation lesions involving a large side branch. In contrast with previous studies, the longer and more complex two-stent procedures did not result in more procedure-related MIs. Prof. Kumsars concluded that longer-term follow-up is needed before the optimal treatment strategy for this type of lesion can be recommended.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.