

Summary
The American College of Cardiology (ACC) and the American Heart Association (AHA) introduced new and/or updated evidence-based clinical practice guidelines in the AHA's journal Circulation and the Journal of the American College of Cardiology. This article provides an overview of the guidelines, which were also presented at the 2013 AHA Scientific Sessions.
- Prevention & Screening
- Obesity
- Cardiology Guidelines
- Lipid Disorders
- Prevention & Screening
- Exclusive Article - For home page
- Obesity
- Cardiology Guidelines
- Cardiology & Cardiovascular Medicine
- Lipid Disorders
The American College of Cardiology (ACC) and the American Heart Association (AHA) introduced new and/or updated evidence-based clinical practice guidelines in the AHA's journal Circulation and the Journal of the American College of Cardiology. This article provides an overview of the guidelines, which were also presented at the 2013 AHA Scientific Sessions.
ASSESSING RISK
Donald M. Lloyd-Jones, MD, ScM, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA, discussed the approach taken to develop the 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk and reviewed some of the key recommendations [Goff DC Jr et al. J Am Coll Cardiol 2013; Circulation 2013].
The objective of this Task Force was to provide an optimal mechanism for clinicians in the United States to accurately estimate risk of first atherosclerotic cardiovascular disease (ASCVD) events in asymptomatic patients. The Task Force examined the current scientific evidence for available risk scores and found several issues, including nonrepresentative derivation populations and narrowly defined endpoints. The decision was made to develop a new risk tool that included cohorts designed to be representative of the US population, are community-or population-based, and include at least 10 years of follow-up including recent data reflecting contemporary risk factor trends and event rates.
The models were developed using pooled data from several large racially and geographically diverse National Heart, Lung, and Blood Institute (NHLBI)-sponsored cohort studies. Data from approximately 25,000 apparently healthy non-Hispanic African American and white men and women free of a previous history nonfatal of myocardial infarction (MI; recognized or unrecognized), stroke, heart failure, percutaneous coronary intervention, coronary artery bypass surgery, or atrial fibrillation were used to develop sex- and race-specific models to predict 10-year risk for coronary heart disease death, nonfatal MI, and fatal and nonfatal stroke.
Risk prediction models that included both traditional and newer risk factors were tested and validated. The c-statistic of the risk prediction model ranged from 0.71 to >0.82 (Table 1).
ASCVD Risk Calculator: Model Characteristics
Table 2 shows the factors included in the calculation of risk.
ASCVD Risk Calculator
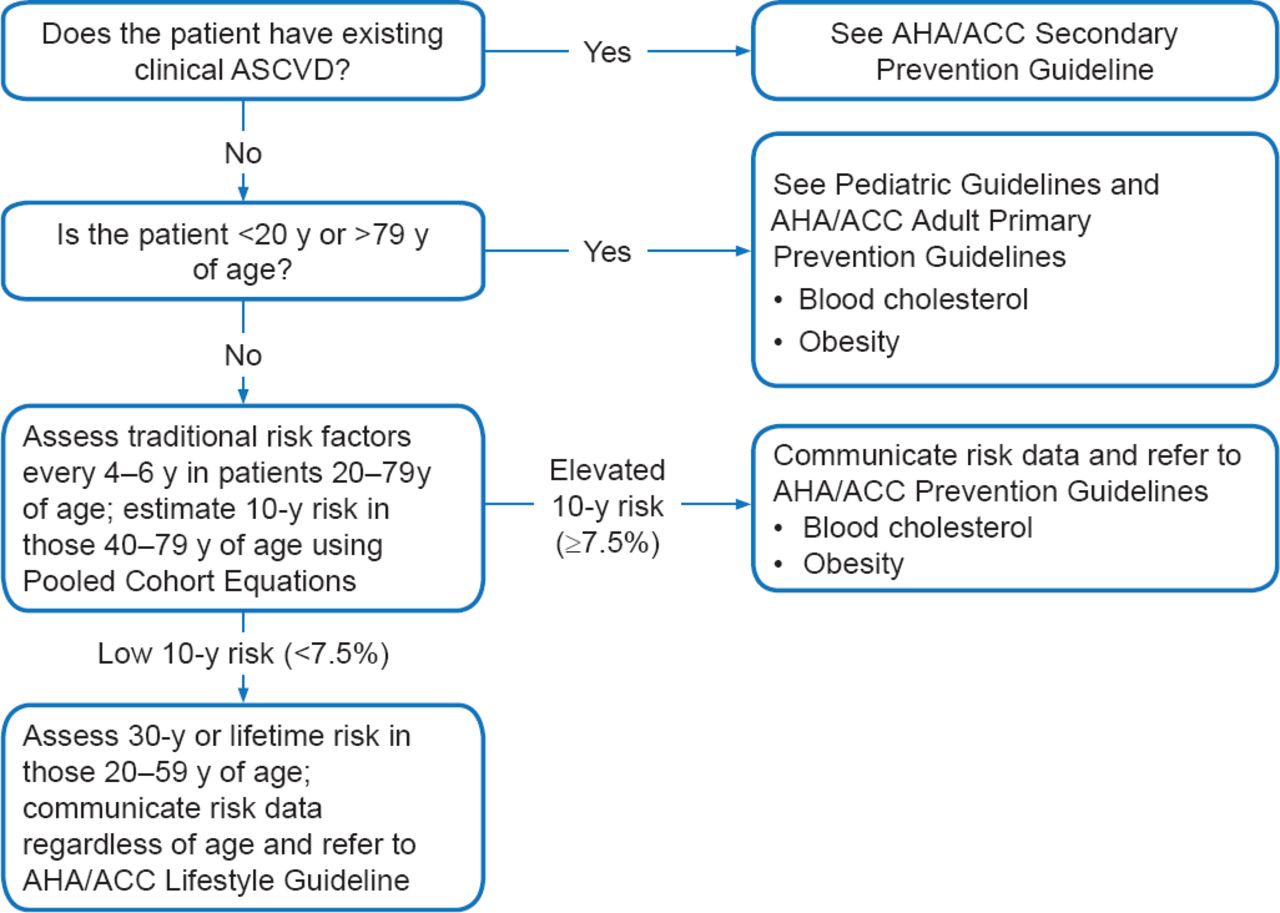
The web-based calculator is available at http://my.americanheart.org/cvriskcalculator and http://www.cardiosource.org/science-andquality/practice-guidelines-and-quality-standards/2013-prevention-guideline-tools.aspx. It is recommended that the race- and sex-specific Pooled Cohort Equations to predict 10-year risk should be used in non-Hispanic, African Americans, and non-Hispanic Whites aged 40 to 79 years (Class I, Level of Evidence [LOE] B). Use of the cohorts for non-Hispanic Whites may be considered when estimating risk in patients from other populations (Class IIb, LOE C). Figure 1 shows how to implement the risk assessment in clinical practice.

Implementation of Risk Assessment Work Group Recommendations
ACC=American College of Cardiology; AHA=American Heart Association; ASCVD=atherosclerotic cardiovascular disease; BMI=body mass index.
Reproduced from Goff DC, Jr et al. ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
The Task Force also addressed several critical questions relevant to clinical practice. Based on their findings, they made the following additional recommendations:
-
In the case of uncertainty after the 10-year risk assessment has been completed, assessment of one or more of the following may be considered to inform treatment decision-making: family history, high-sensitivity C-reactive protein (hs-CRP), coronary artery calcium (CAC), or ankle-brachial index (ABI; Class IIb, LOE B)
-
Carotid intima-media thickness is not recommended for routine measurement in clinical practice for risk assessment for a first ASCVD event (Class III, LOE B)
In terms of long-term ASCVD risk estimation, the Task Force recommends reassessment of traditional ASCVD risk factors every 4 to 6 years in adults aged 20 to 70 years who are free from ASCVD and to estimate 10-year risk every 4 to 6 years in adults aged 40 to 79 years without ASCVD (Class IIa, LOE B). Clinicians may consider assessing 30-year or lifetime ASCVD risk based on traditional risk factors in adults aged 20 to 59 years who are free of ASCVD and not at short-term risk (Class IIb, LOE C).
TREATMENT OF BLOOD CHOLESTEROL
Neil Stone, MD, MACP, Northwestern Memorial Hospital, Chicago, Illinois, USA, discussed the goals of the Task Force in preparing the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults and presented an overview of its key points [Stone NJ et al. J Am Coll Cardiol 2013; Circulation 2013].
Key questions addressed in the preparation of this guideline were the usefulness of low-density lipoprotein (LDL) and non-high-density lipoprotein (HDL) targets in the management of cholesterol to reduce ASCVD risk and the identification of groups of individuals most likely to benefit from cholesterol-lowering therapy. The group also examined the efficacy and safety of the available lipid drugs and offered clinical guidance.
The recommendations in this guideline are based on evidence from randomized controlled clinical trials (RCTs) and systematic reviews/meta-analyses of RCTs that were independently assessed for quality. For patients without ASCVD or primary elevations of LDL-C ≥190 mg/dL, the guideline recommends use of the new risk prediction model (described above) to assess 10-year ASCVD risk in both white and black men and women to guide the initiation and/or intensity of statin therapy.
Titration of drug therapy to specific LDL-C and/or non-HDL-C goals was not recommended by the Task Force due to lack of RCT evidence demonstrating benefit of this approach. Instead the treatment principles in this guideline are based on strong RCT evidence for the use of appropriate intensity of statin therapy to reduce the risk of ASCVD in individuals who are most likely to benefit. Four statin benefit groups were identified:
-
Individuals with clinical ASCVD
-
Individuals with primary elevations of LDL-C ≥190 mg/dL
-
Individuals aged 40 to 75 years with diabetes and LDL-C 70 to 189 mg/dL
-
Individuals without clinical ASCVD or diabetes who are 40 to 75 years of age with LDL-C 70–189 mg/dL and an estimated 10-year ASCVD risk of 7.5% or higher (NOTE: ASCVD risk and appropriateness of therapy should be discussed with individual patients prior to initiation of statin therapy)
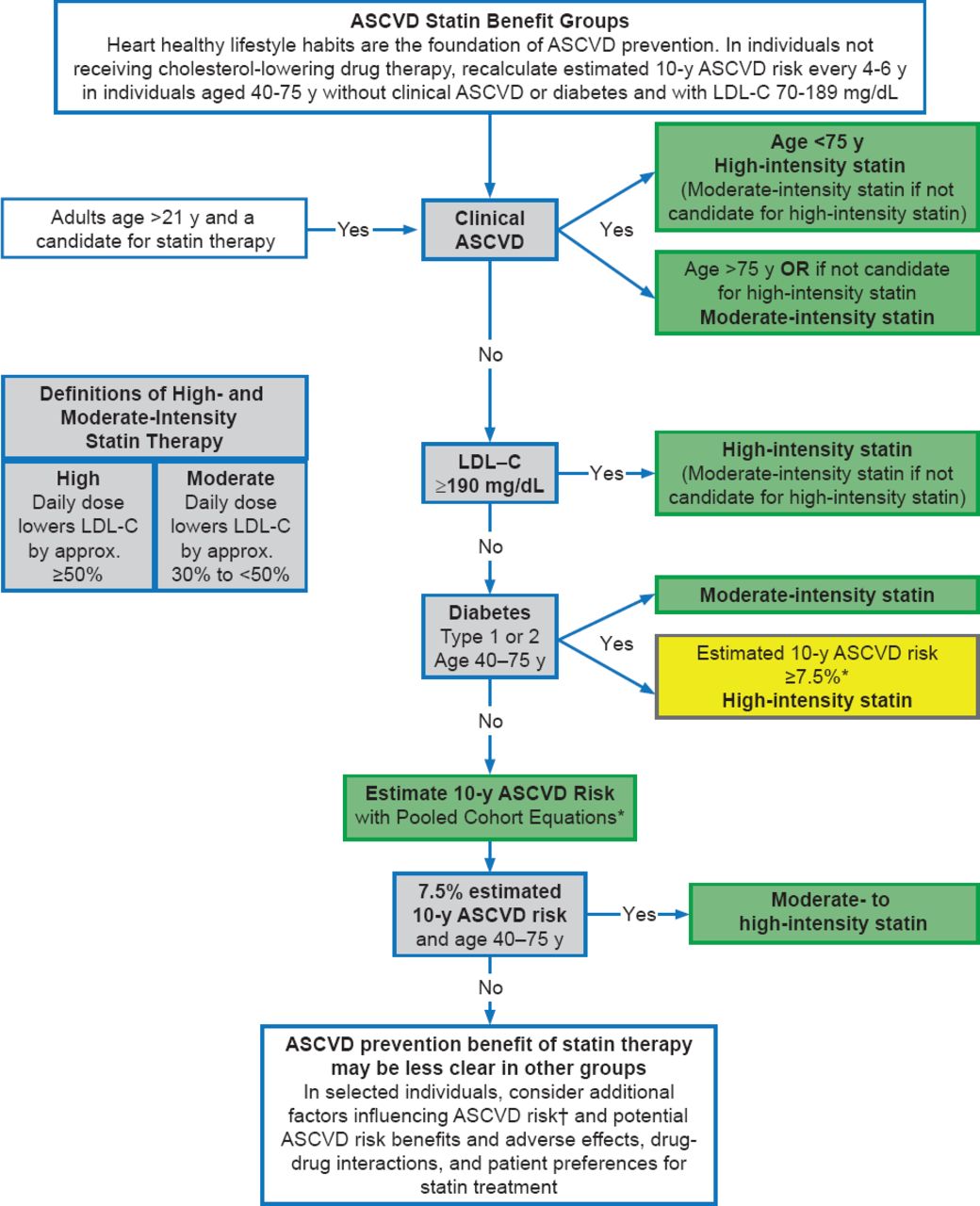
Recommendations on intensity of statin treatment for each group are summarized in Figure 2. The definitions of high-, moderate-, and low-intensity therapy are shown in Table 3. The panel could find no data supporting the routine use of non-statin drugs combined with statin therapy to further reduce ASCVD events. The panel recommended against routine use of such combination therapy except for patients with familial hypercholesterolemia.
Definition of High-, Moderate-, and Low-Intensity Statin Therapy*

Major Recommendations for Statin Therapy for ASCVD Prevention
Colors correspond to the class of recommendations in the ACC/AHA Table 1. This flow diagram is intended to serve as an easy reference guide summarizing recommendations for ASCVD risk assessment and treatment. Assessment of the potential for benefit and risk from statin therapy for ASCVD prevention provides the framework for clinical decision making incorporating patient preferences.
*Percent reduction in LDL-C can be used as an indication of response and adherence to therapy, but is not in itself a treatment goal.
†Primary LDL-C ≥160 mg/dL or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, high-sensitivity C-reactive protein >2 mg/L, CAC score ≥300 Agatston units or ≥75 percentile for age, sex, and ethnicity, ankle-brachial index <0.9, or elevated lifetime risk of ASCVD
ASCVD=atherosclerotic cardiovascular disease; CAC=coronary artery calcium; LDL-C=low-density lipoprotein cholesterol; y=year(s).
Reproduced from Stone NJ et al. ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
The guideline did indicate that clinicians treating high-risk patients who have a less-than-anticipated response to statins, who are only able to tolerate less-than recommended intensity of a statin, or who are completely statin-intolerant may consider the addition of non-statin, cholesterol-lowering therapy. High-risk individuals were defined as those with ASCVD, those with LDL-C ≥190 mg/dL and those with diabetes. The guideline recommends clinicians integrate patient preferences and select drugs that have been shown in RCTs to provide ASCVD risk-reduction benefits that outweigh the potential for adverse effects and limit drug-drug interactions.
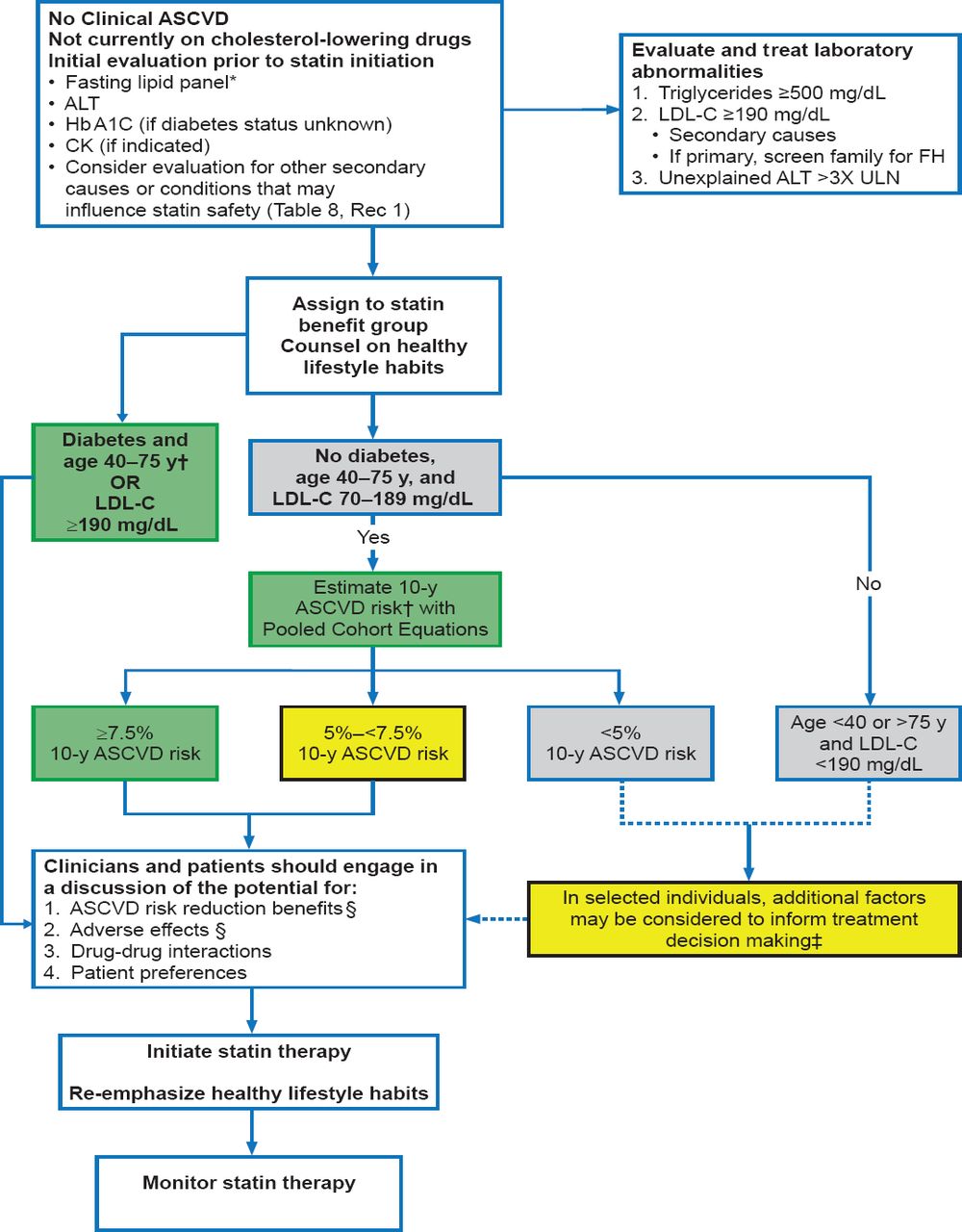
It should be noted in Figure 3 that statins are not automatically prescribed if a primary prevention individual has a ≥7.5% ASCVD risk. Rather what is recommended is that a clinician-patient discussion occur to determine patient's risk characteristics, consider the ASCVD risk reduction benefits and negative aspects of statin therapy including drug-drug interactions, and incorporate patient preferences into decision-making. This discussion could highlight other risk factors of importance such as elevated blood pressure and tobacco usage as well as determine if statin therapy should be started. This discussion should also include patient preference in those situations where a patient without significant risk factors other than age had an ASCVD risk ≥7.5%. Here, a shared decision-making process may result in forgoing statin therapy despite increased risk.

Primary Prevention: Initiating Statin Therapy
Colors correspond to the class of recommendations in the ACC/AHA Table 1.
*Fasting lipid panel preferred. In a nonfasting individual, a nonfasting non-HDL-C >220 mg/dL may indicate genetic hypercholesterolemia that requires further evaluation or a secondary etiology. If nonfasting triglycerides are >500 mg/dL, a fasting lipid panel is required.
†The Pooled Cohort Equations can be used to estimate 10-year ASCVD risk in individuals with and without diabetes.
A downloadable spreadsheet enabling estimation of 10-year and lifetime risk for ASCVD and a web-based calculator are available at http://my.americanheart.org/cvriskcalculator and http://www.cardiosource.org/science-and-quality/practice-guidelines-and-quality-standards/2013-prevention-guideline-tools.aspx.
‡These factors may include primary LDL-C >160 mg/dL or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, sensitivity-C-reactive protein >2 mg/L ≥300 Agatston units or ≥75 percentile for age, sex, and ethnicity (For additional information, see http://www.mesa-nhlbi.org/CACReference.aspx), ABI <0.9, or lifetime risk of ASCVD. Additional factors that may aid in individual risk assessment may be identified in the future.
§1) Potential ASCVD risk reduction benefits (e.g., absolute risk reduction from moderate- or high-intensity statin therapy can be approximated by using the estimated 10-year ASCVD risk and the relative risk reduction of ∼30% for moderate-intensity statin or ∼45% for high-intensity statin therapy. 2) Potential adverse effects. The excess risk of diabetes is the main consideration in ∼0.1 excess case per 100 individuals treated with a moderate-intensity statin for 1 year and ∼0.3 excess cases per 100 individuals treated with a high-intensity statin treated patients for 1 year. Note: a case of diabetes is not considered equivalent to a fatal or nonfatal MI or stroke. Both statin-treated and placebo-treated participants experienced the same rate of muscle symptoms. The actual rate of statin-related muscle symptoms in the clinical population is unclear. Muscle symptoms attributed to statin should be evaluated in Table 8, Safety Rec 8.
ABI=ankle-brachial index; ALT=alanine transaminase; ASCVD=atherosclerotic cardiovascular disease; CK=creatine kinase; FH=familial hypercholesterolemia; LDL-C=low-density lipoprotein cholesterol; ULN=upper limit of normal.
Editor's Note: All references to other figures and tables within this image refer to items in the original published guidelines as cited below.
Reproduced from Stone NJ et al. ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
For individuals not included in the four statin benefit groups, additional factors may inform treatment decisions. There is moderate evidence that there is a net benefit from moderate intensity statin therapy in individuals with 5 to <7.5% 10-year ASCVD risk. In addition, other factors can be considered, including a family history of premature ASCVD, elevated lifetime risk of ASCVD, LDL-C ≥160 g/dL, hs-CRP ≥2.0 mg/L, and the presence of subclinical atherosclerosis (CAC score ≥300 or ABI <0.9). There should also be a discussion of the potential for ASCVD risk reduction benefit, adverse effects, and drug-drug interactions as well as patient preferences prior to a final decision. Thus, a patient with a positive family history or an LDL-C in the 160–189 mg/dL range could be considered for the statin therapy.
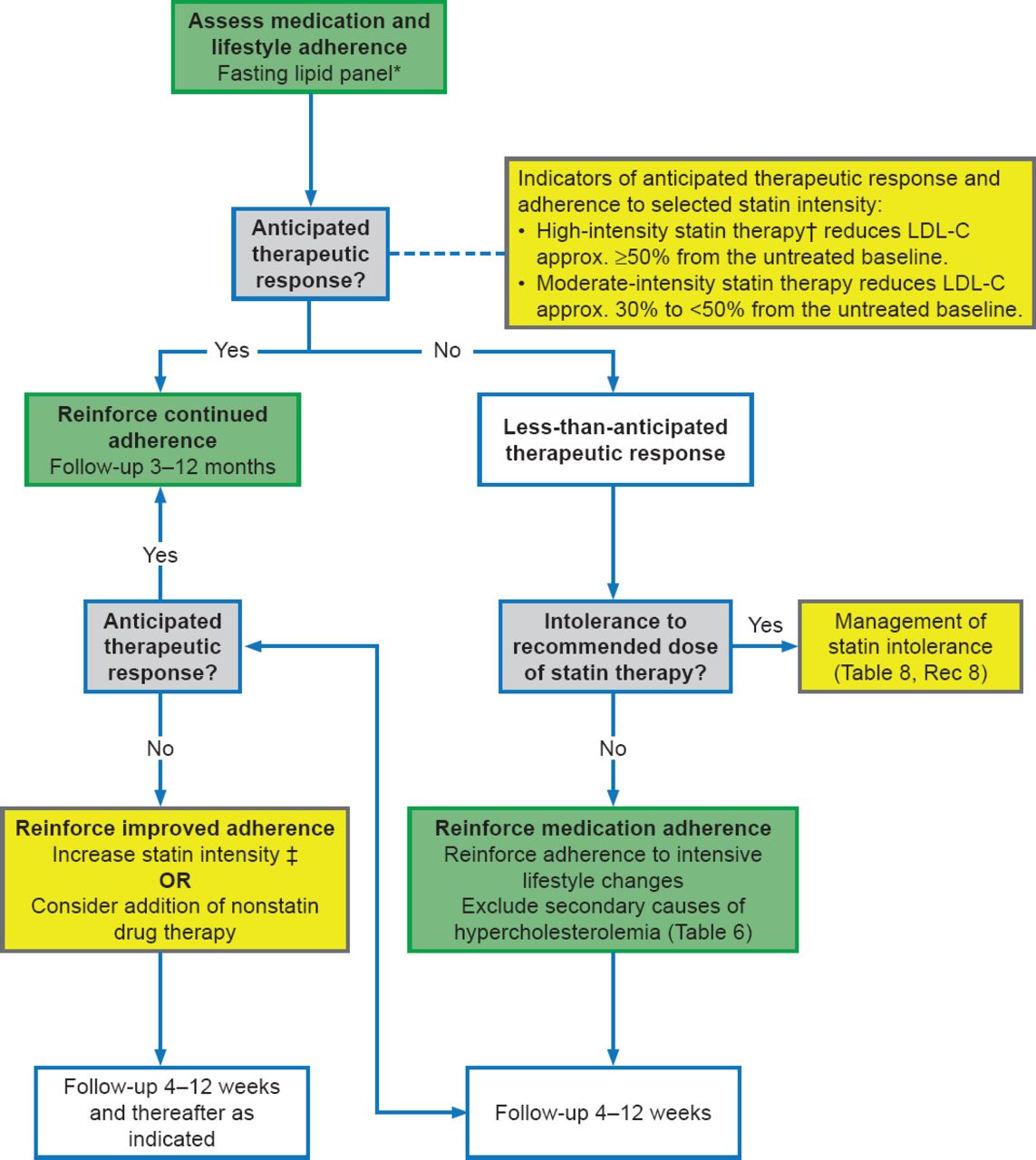
Adherence to the prescribed medication regimen and lifestyle recommendations (eg, diet, exercise, tobacco use) should be assessed using a fasting lipid panel as clinically indicated for the individual patient. The key measure for assessing adherence is whether the patient has achieved the anticipated reduction of LDL-C (see Table 3 for specifics). Figure 4 shows that a fasting lipid panel and if needed, safety assessments, are evaluated at appropriate intervals in follow-up. In those already taking a statin, in whom the baseline LDL-C is unknown, the guidelines noted that an LDL-C <100 mg/dL was observed in most individuals receiving high-intensity statin therapy in RCTs.

Statin Therapy: Monitoring Response and Adherence
Colors correspond to the class of recommendations in the ACC/AHA Table 1.
*Fasting lipid panel preferred. In a nonfasting individual, a nonfasting non-HDL-C >220 mg/dL may indicate genetic hypercholesterolemia that requires further evaluation or a secondary etiology. If nonfasting triglycerides are >500 mg/dL, a fasting lipid panel is required.
†In those already on a statin, in whom baseline LDL-C is unknown, an LDL-C <100 mg/dL was observed in most individuals receiving high-intensity statin therapy in RCTs.
‡In those already on a statin, in whom the baseline LDL-C is unknown, an LDL-C <100 mg/dL was observed in most individuals receiving high-intensity statin therapy in RCTs. For further review see Section 6.3.1 of the guidelines.
ASCVD=atherosclerotic cardiovascular disease; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; RCT=randomized clinical trial
Editor's Note: All references to other figures and tables within this image refer to items in the original published guidelines as cited below.
Reproduced from Stone NJ et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
The guideline provides specific advice on the evaluation of muscle symptoms and on other safety considerations. Dr. Stone concluded by noting that the guidelines used a strict, evidence-based, process to match the guidelines more closely to the existing scientific evidence. The emphasis is on drug therapies proven to reduce ASCVD events rather than solely to lower cholesterol. The Task Force identified 4 groups of individuals most likely to benefit from statin therapy based on an extensive body of RCT evidence that showed a reduction in ASCVD events with a good margin of safety. To address the large burden of ASCVD in a country where almost one in three die of CVD, the Task Force has presented a strategy for primary prevention that uses a representative risk calculator to predict ASCVD risk and includes share decision making between the clinician and the patient to determine the optimal treatment approach.
OBESITY AND LIFESTYLE
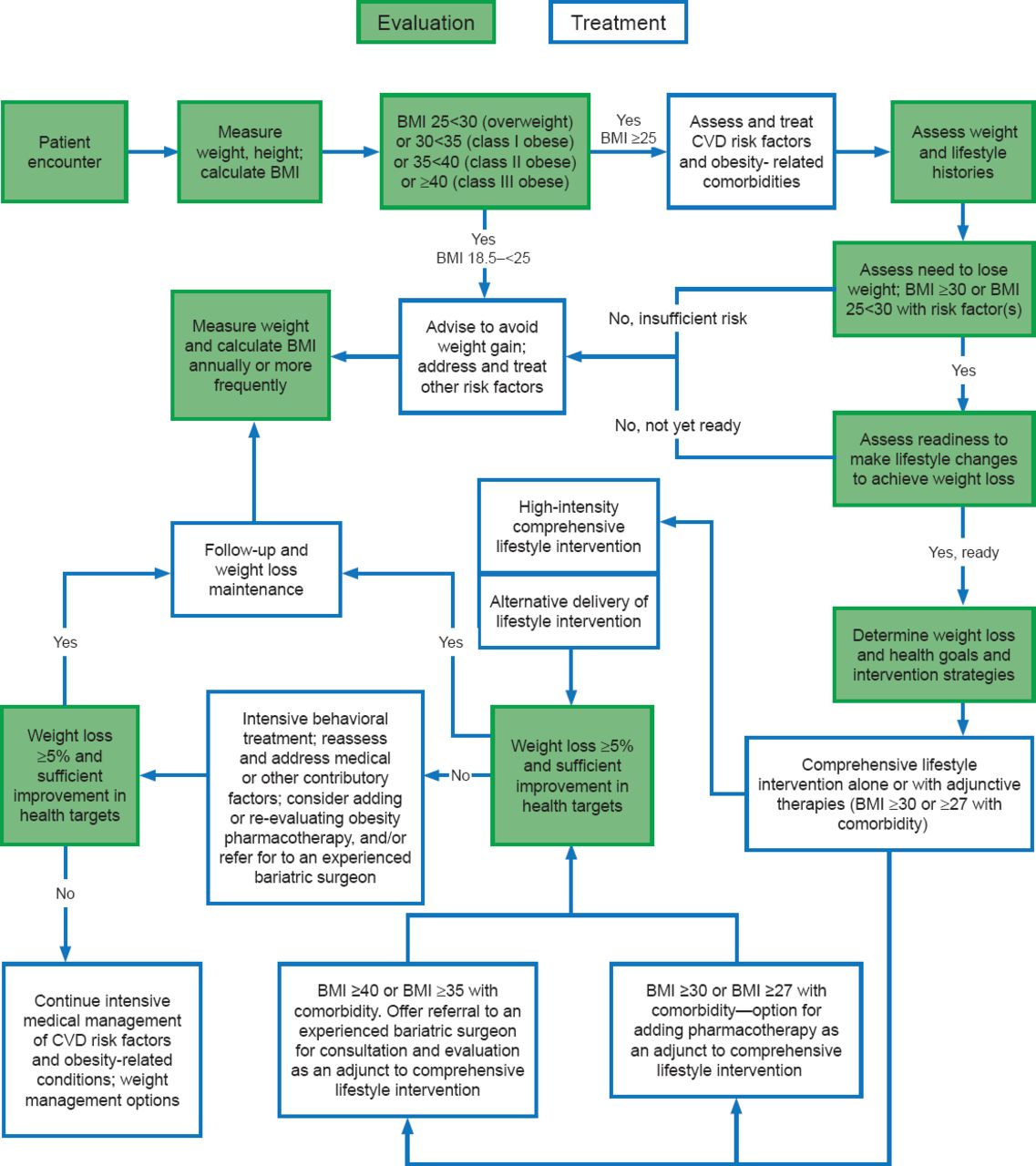
High-quality treatments that can lead to medically important weight loss are available. However, the ability of primary care providers (PCPs) to manage patients who need to lose weight is often compromised by a lack of training in the management of obesity. Donna H. Ryan, MD, Pennington Biomedical Research Center in Baton Rouge, Louisiana, United States, discussed the 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults [Jensen MD et al. J Am Coll Cardiol 2013; Circulation 2013], which is geared specifically to PCPs.
The guidelines include a treatment algorithm (Figure 5) and focus on 5 critical recommendations. The first of these is the identification of individuals who need to lose weight. Under the new guidelines weight loss treatment is indicated for obese individuals (body mass index [BMI] ≥30 kg/m2) and overweight (BMI >25.0 to 29.9 kg/m2) individuals with ≥1 indicators of increased cardiovascular risk (eg, DM, pre-DM, hypertension, dyslipidemia, elevated waist circumference [WC]) or other obesity related comorbidities (Class I, Level of Evidence [LOE] B).

Chronic Care Model of Weight Management by Primary Care Providers
BMI=body mass index; CVD=cardiovascular disease; FDA=Food and Drug Administration.
†BMI cut-point determined by the FDA and listed on the package inserts of FDA-approved obesity medications.
Editor's Note: This algorithm applies to the assessment of overweight and obesity in adults and subsequent decisions based on that assessment. Each step (designated by a box) in this process is reviewed in this section and expanded upon in subsequent sections within the original guidelines article as cited below.
Reproduced from Jensen MD et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
The panel recommends that patients be counseled concerning the benefits of weight loss. Although the usual recommendation is to aim for a weight loss goal of 5% to 10%, patients should be informed that clinically meaningful benefits in triglyceride levels and DM risk can be achieved with lifestyle changes that produce sustained weight loss reductions of as little as 3% to 5%, and greater amounts of weight loss will reduce blood pressure, improve LDL-C and HDL-C and reduce the need for medications to control blood pressure, blood glucose and lipids as well as further reduce triglycerides and blood glucose (Class I, LOE A). Patients do not need to achieve a BMI <25 to achieve health benefits.
In terms of the best diet for weight loss, the panel did not single out one diet as superior, as what seems to be important in weight loss is achieving and sustaining a calorie deficit. Therefore, the panel recommends that the diet recommendation be part of comprehensive lifestyle intervention geared to create a calorie deficit through diet and physical activity (Class I, LOE A). The calorie reduced diet choice should be based on the patient's preferences and health status and physicians should preferably refer to a nutrition professional for counseling.
The centerpiece of the new recommendations, noted Dr. Ryan, is the recommendation that patients who need to lose weight should receive a comprehensive program (diet, physical activity, and behavior modification) lasting ≥6 months. The program ideally should be an onsite, high intensity (>14 sessions in 6 months), comprehensive intervention delivered in group or individual sessions by a trained interventionist and persisting for at least 1 year (Class I, LOE A). When necessary, other approaches (ie, web or telephone based) may be used although the amount of weight loss may be less (Class IIa, LOE A).
Patients with a BMI ≥35 kg/m2 and a comorbidity or a BMI ≥40 kg/m2 should be advised that bariatric surgery may be an appropriate option and physicians should offer referral to an experienced bariatric surgeon for consultation and evaluation (Class IIa, LOE A).
Dr. Ryan noted that there are several gaps in the guidelines, including the absence of critical questions on pharmacotherapy, physical activity protocols, and medication related weight gain. There is also a need for an evidence review for WC and BMI as categorical variables to establish additional recommendations regarding cut points.
The importance of lifestyle interventions in the reduction of cardiovascular risk cannot be overstated. Robert H. Eckel, MD, University of Colorado, Aurora, Colorado, United States, reviewed the evidence review of the effects of dietary patterns, sodium and potassium intake, and physical activity on BP and lipids among normal, overweight, and obese adults compared with either no treatment or other types of interventions.
Strong evidence from two RCTs shows the DASH diet to be associated with reductions in BP and LDL-C (Table 4). The effect of the DASH diet on lowering both BP and lipids were consistent for women and men, African American and non-African Americans, older and younger adults, and hypertensive and non-hypertensive adults. The committee also evaluated the Mediterranean Diet and high- versus low-glycemic diets. They found the Mediterranean Diet to be consistent with a good dietary pattern. Although the strength of evidence is low, the Mediterranean diet was associated with reductions in BP (6–7/2–3 mm Hg in middle-aged or older adults with type 2 DM mellitus or ≥3 cardiovascular risk factors and by 2–3/1–2 mm Hg in healthy younger adults). They found no consistent effect of the diet on lipids. In addition, the committee examined three RCTs evaluating glycemic index and determined that there is insufficient evidence to determine whether low- versus high-glycemic diets affect lipids or BP for adults without DM. The evidence for this relationship in adults with DM was not reviewed.
Effect of DASH Diet on Blood Pressure and Lipids*
The committee recommends that adults who would benefit from LDL-C and BP lowering be advised to adhere to a dietary pattern emphasizing vegetables, fruits, and whole grains, which includes low-fat dairy products, poultry, fish, legumes, non-tropical vegetable oils and nuts and limits intake of sweets, sugar-sweetened beverages, and red meats. This dietary pattern should be adapted to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions. The DASH diet, the USDA Food Pattern, and the AHA Diet are recommended (Class Ia, LOE A).
The committee felt that there are an insufficient number of studies in the appropriate population to determine whether lowering dietary cholesterol reduces LDL-C. For saturated fats, however, there is convincing evidence that a dietary pattern, which achieves a macronutrient composition of 5% to 6% saturated fat, 26% to 27% total fat, 15% to 18% protein, and 55% to 59% carbohydrate is associated with reductions in LDL-C (11 to 13 mg/dL in 2 studies; 11% in a another study). There is moderate evidence in favor of replacing trans-fats with other fats to reduce LDL-C and triglycerides and increase HDL-C. Adults who would benefit from LDL-C lowering should aim for a dietary pattern that achieves 5% to 6% of calories from saturated fat, and reduce the percent of calories from saturated and trans-fat (Class Ia, LOE A).
There is a high level of evidence showing that among adults aged 25 to 80 years with BP 120–159/80–95 mm Hg, reducing sodium intake lowers BP. Among adults with prehypertension or hypertension, reducing sodium intake lowers BP in women and men, African American and non-African American adults, and older and younger adults. Adults who would benefit from BP lowering should lower their sodium intake (Class I, LOE A). They should be advised to consume no more than 2400 mg/day of sodium. Further reduction of sodium intake to 1500 mg/day is associated with an even greater reduction in BP. Reducing sodium by at least 1000 mg/day will lower BP, even if the target daily sodium intake is not yet achieved (Class IIa, LOE B).
Among adults, aerobic physical activity is associated with a 3.0 to 6.0 mg/dL reduction in LDL-C and an average reduction in non-HDL-C of 6.0 mg/dL. There was no consistent effect on HDL-C or triglycerides. Resistance training for ≥3 days/week for 24 weeks in duration that includes 9 exercises performed for 3 sets and 11 repetitions at an average intensity of 70% of 1-maximal repetition is associated with reductions of 6.0 to 9.0 mg/dL in LDL-C, triglycerides, and non-HDL-C. There is no effect on HDL-C. In general, adults needed to lower their LDL-C and non-HDL-C should engage in aerobic physical activity involving moderate-to-vigorous intensity physical activity 3 to 4 times/week for an average of 40 minutes per session (Class IIa, LOE B).
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.