

Summary
This article outlines the rational, objectives, and methodology of the second Diabetes Attitudes Wishes and Needs study [DAWN2; Peyrot M et al. Diabetes Res Clin Pract 2013]. A major impetus for DAWN2 was the growing incidence of diabetes—now labeled a worldwide epidemic—and a desire to gain insight into what has changed with respect to the management of diabetes since the original DAWN study in 2001, how individuals with diabetes perceive their disease, and the societal environments that surround people with diabetes.
- Diabetes Mellitus
- Mood Disorders
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
- Mood Disorders
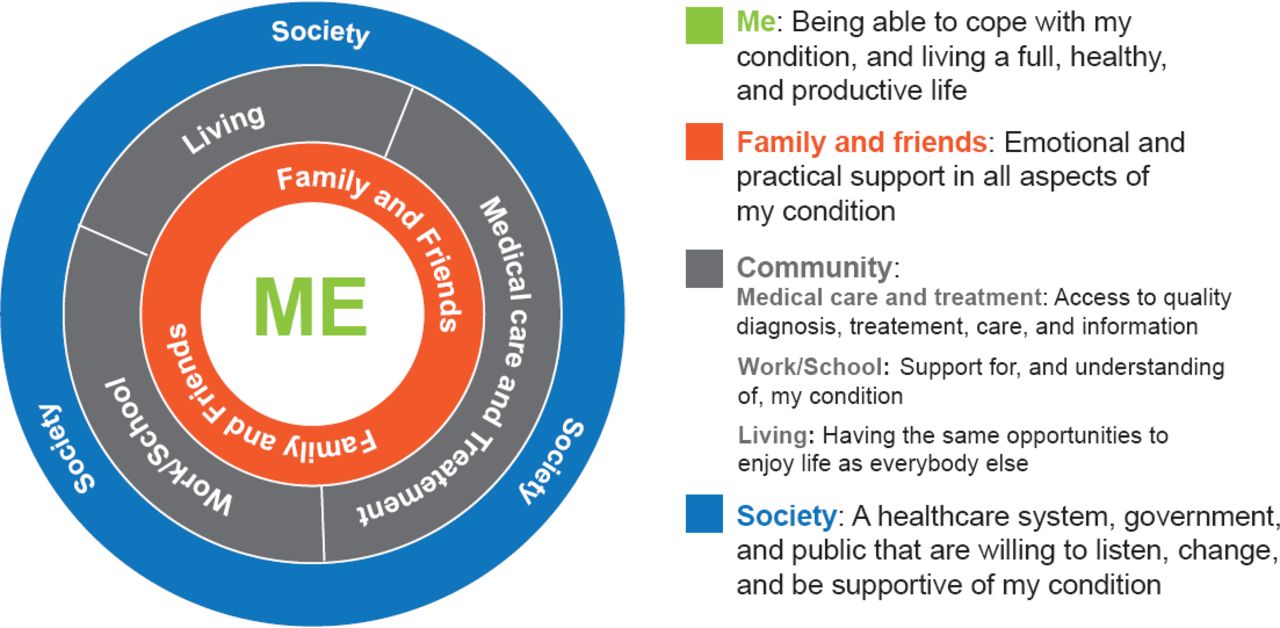
Mark Peyrot, PhD, Loyola University, Baltimore, Maryland, USA, trial head, outlined the rational, objectives, and methodology of the second Diabetes Attitudes Wishes and Needs study [DAWN2; Peyrot M et al. Diabetes Res Clin Pract 2013]. A major impetus for DAWN2 was the growing incidence of diabetes—now labeled a worldwide epidemic—and a desire to gain insight into what has changed with respect to the management of diabetes since the original DAWN study in 2001, how individuals with diabetes perceive their disease, and the societal environments that surround people with diabetes. The model of diabetes used in DAWN2 is person-centered, involving family and friends, the community, and society (Figure 1).

DAWN Needs Model for Diabetes
Source: http://www.dawnstudy.com/dawn2/dawn-2-study-design.asp.
The primary objective of DAWN2 was to assess potential barriers to and facilitators of active and successful management of diabetes among people with diabetes, their family members, and healthcare professionals [Peyrot M et al. Diabetes Res Clin Pract 2013]. Other goals were to establish national benchmarking standards for health status, quality of life (QoL), and access to self-management education and self-care; assess access to, use of, and benefit from various support systems; identify important facilitators and barriers to person-centered care for each stakeholder group, and quantify the successes, wishes, needs, preferences, and priorities for all key stakeholders in diabetes.
DAWN2 surveyed >16,000 individuals in 17 countries across 4 continents between March and September 2012 (Table 1). Respondents completed group-specific questionnaires predominantly online or by telephone interview, supplemented by face-to-face interviews in some countries. Topics covered in the questionnaire included health and QoL, attitudes and beliefs about diabetes, training (healthcare professionals), diabetes profile, care and support/involvement, future needs, active self-management, diabetes education and information, and demographic and practice characteristics. Questions from the original DAWN study were included for evaluation of trends. New questions were added to address the issue of discrimination and diabetes education.
Study Population
Stakeholders were identified as adults (aged ≥18 years) with type 1 or 2 diabetes for at least 12 months (treated and not treated); adult family members involved in the care of the an adult with diabetes; and healthcare professionals, in practice for ≥1 year who treat people with diabetes (primary care/general practitioners, diabetes specialists, nurses/nurse educators, dietitians/nutritionists).
Benchmarking was an important component of the study meant to provide an empirical standard by which participating countries could assess their existing QoL and person-centered quality care, in order to track progress over time and identify areas of unmet need. It would also allow for cross-national comparisons by which countries can assess their outcomes relative to other countries, identify diabetic care models for best practices, and perhaps identify areas for collaboration.
Frans Pouwer, MS, PhD, Tilburg University, Tilburg, The Netherlands, presented findings from the DAWN2 study [Holt RI et al. Diabet Med 2013; Kovacs Burns K et al. Diabet Med 2013; Nicolucci A et al. Diabet Med 2013]. The study revealed that diabetes is a major psychosocial burden for patients and their families, but there are opportunities for improving care, education, and psychosocial support. There is a need for broad dialogue and collaborative action to raise the voices of people with diabetes and improve their health and QoL. This can best be accomplished by putting people and their families' center stage in the treatment process.
Depression is common in persons with diabetes; occurring 2 to 3 times more frequently compared with nondiabetic individuals. In the 17-country survey, the proportion of diabetic individuals with likely depression (WHO-5 Well-Being Index [WHO-5] score ≤28) was 13.8% (country range, 6.5% to 24.1%) [Nicolucci A et al. Diabet Med 2013].
Diabetes-related distress (Problem Areas in Diabetes Scale 5 score [PAID-5] ≥40) was reported by 44.6% of participants (range, 17.2% to 67.6%) with Southern and Eastern Europe and Asia having higher than mean PAID-5 scores [Nicolucci A et al. Diabet Med 2013]. Approximately 40% of participants (range, 18.6% to 64.9%) reported that their antidiabetic medication interfered with their ability to live a normal life and 55.5% said they felt very worried about the risk of hypoglycemia. Diabetes had a negative impact on all aspects of QoL: 20.5% of respondents said it had a negative impact on relationship with family/friends, a negative impact on work and studies (35.4%), on leisure activities (38.2%), on finances (44.0%), emotional well-being (46.2%), and physical health (62.2%).
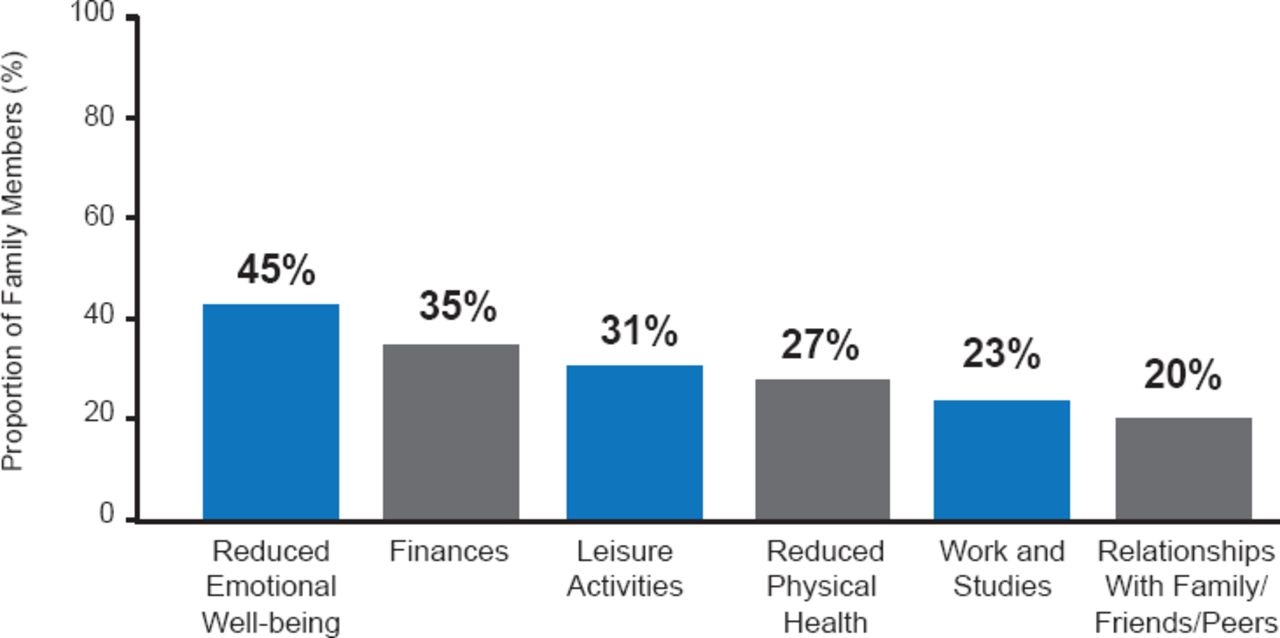
QoL of the family members caring for the person with diabetes was also impacted. Family members (35.3%; range, 10.6% to 61.7%) reported a moderate to very large burden caring for a relative with diabetes [Kovacs Burns K et al. Diabet Med 2013]. Family members reported a negative impact on physical health (26%), emotional well-being (45%), finances (35%), leisure activity (31%), work and studies (23%), and relationships with family and friends (20%; Figure 2).

Impact of Diabetes on Lives of Family Members
Source: Kovacs Burns K et al. Diabet Med 2013.
Over half of respondents (51.4%; range, 22.5% to 76.0%) rated their QoL as ‘good’ or ‘very good’. Family members also worried about the risk of hypoglycemia (61.3%; range, 31.5% to 86.4%) in the diabetic person under their care.
A low rating was given to the availability of person-centered chronic illness care and support for active self-involvement. Following self-care advice for medication and diet was most common among respondents, and following advice for glucose monitoring and foot examination was least common. A marked variation was noted between countries [Nicolucci A et al. Diabet Med 2013]. Healthcare professionals voiced a need for more people with diabetes to be involved in self-care (range, 61.4% to 92.9%) [Holt RI et al. Diabet Med 2013]. Glucose monitoring (range, 29.3% to 92.1%) had the biggest country difference, with a between-country variance of 20%. Major improvement needs in diabetes self-management education was reported by 60% (26.4% to 81.4%) of healthcare professionals (12% between-country variance). Only 48.8% of respondents had participated in diabetes educational programs/activities to help manage their diabetes [Nicolucci A et al. Diabet Med 2013], although most who participated in an educational program found them helpful (72.1%; range, 42.1% to 90.3%) [Kovacs Burns K et al. Diabet Med 2013].
People with diabetes and their healthcare professionals felt there was a need for more psychological support (62.7%; range, 40.6% to 79.6%) [Holt RI et al. Diabet Med 2013]. Many healthcare professionals indicated that major improvements were needed in the provision of diabetes services, which differed among countries. Suggestions included healthcare organizations (30.6%; range, 7.4% to 67.1%), resources for diabetes prevention (78.8%; range, 60.4% to 90.5%), earlier diagnosis and treatment (67.9%; range, 45.0% to 85.5%), communication between team members and people with diabetes (56.1%; 22.3% to 85.4%), and specialist nurse availability (63.8%; range, 27.9% to 90.7%). In some countries, up to one third of healthcare professionals reported not having received any formal diabetes training and 59% would like more training in this area.
Societal discrimination against people with diabetes was reported by 32.8% (11.4% to 79.6%) of participants [Holt RI et al. Diabet Med 2013] and was associated with diabetes-related distress. Many family members (21.5%) also felt diabetes-related discrimination was a problem [Kovacs Burns K et al. Diabet Med 2013]. Globally, 19.2% of people with diabetes felt discriminated against because of their diabetes [Wens J et al. EASD 2013 (abstr 1102)].
The 5th International DAWN Summit in April 2014 will bring together stakeholders from all DAWN2 countries to learn from each other and develop national action plans.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.