

Summary
This article discusses potential drug/disease interaction between the glucagon-like peptide-1 (GLP-1)-based diabetic therapies and pancreatitis (acute and chronic) and pancreatic cancer.
- Gastrointestinal Cancers
- Diabetes Mellitus
- Gastrointestinal Cancers
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
Fred Gorelick, MD, Yale University and Connecticut Veterans Administration Health Care, New Haven, Connecticut, USA, discussed potential drug/disease interaction between the glucagon-like peptide-1 (GLP-1)-based diabetic therapies and pancreatitis (acute and chronic) and pancreatic cancer.
The pathogenesis of pancreatitis and pancreatic cancer is comprised of complex and sequential insults that converge to cause disease. In the case of acute pancreatitis, these factors can also affect its severity. The risk of developing acute pancreatitis is ∼1.5- to 3-fold higher among individuals with diabetes. Diabetes is also an important finding among individuals with chronic pancreatitis, especially of long (∼15 years) duration [Lankisch PG. Pancreatology 2001]. Diabetes (long-term or adult onset) increases the risk for developing pancreatic cancer [Yeo TP, Lowenfels AB. Cancer J 2012] and pancreatic cancer can cause diabetes [Sah RP et al. Nat Rev Gastroenterol Hepatol 2013].
Over 500 drugs have been associated with pancreatitis, but only about one tenth have been shown to cause disease with rechallenge. With the exception of drugs that dramatically increase serum triglyceride levels, the mechanism of drug-induced pancreatitis is largely unknown. A few drugs, such as insulin, may increase the risk of pancreatic cancer. Several theoretical mechanisms have been proposed for drug-induced pancreatic disease (Table 1).
Theoretical Mechanisms by Which Drugs Might Increase Pancreatic Disease
There are several characteristics of the GLP1 receptors (GLP1-R) that could be related to pancreatic disease. They are localized in neuronal and epithelial tissue in the small intestine and could affect intestinal permeability and increase the access of damaging bacterial products, such as LPS, to the circulation. At least one study has shown that GLP-2 agonists can affect the microbiome population, another potentially important factor in pancreatitis, but this has not been examined with GLP1-R. Another consideration is that the pattern of receptor stimulation (meaning both the duration and amplitude of stimulation) can dramatically affect receptor signaling. In this context, GLP-1 agonists are often associated with persistent stimulation that contrasts with the transient receptor activation that occurs physiologically. The potential also exists for off-target effects of GLP-1 agonists such as activation of unrelated receptors and pathways. Finally, there is at least a theoretical concern that GLP1-R could increase the risk of gallstone disease and biliary pancreatitis.
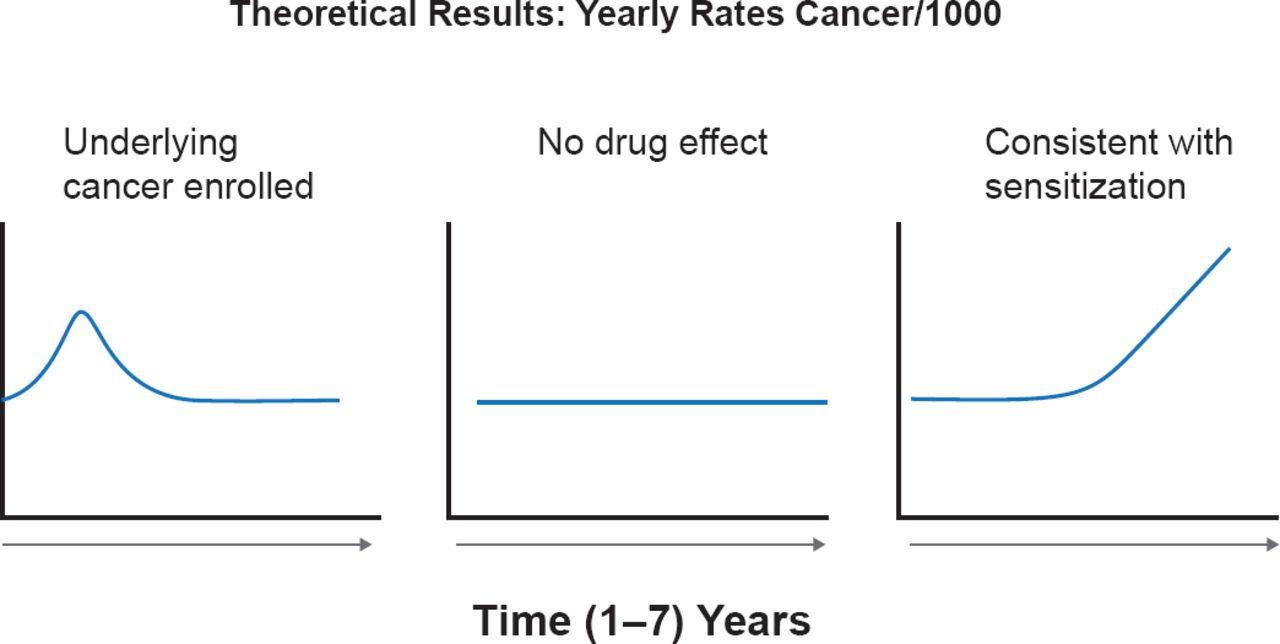
Some literature indicates that antidiabetic drugs, especially those that elevate insulin levels, might increase the risk of pancreatic cancer [Li D et al. Gastroenterology 2009; Bodmer M et al. Am J Gastroenterol 2012]. Some recent data suggested that GLP-1 therapy might increase cell proliferation [Butler PC et al. Diabetes Care 2013]. Dr. Gorelick, speculated that if a GLP1-related or other type of drug increases the risk of pancreatic neoplasia over the short term (2 to 4 years), it is most likely acting synergistically with underlying pathology, such as mutations in the Ras protein. He suggested that in addition to tabulating the total risk at the end of a study, that pancreatic cancer data should be plotted as incidence versus time to more meaningfully suggest causality (Figure 1). Thus, the pattern in the graph to the left with the early peak of cancer occurrence, might suggest that an excess of patients with unsuspected cancer had been enrolled. A flat line would suggest the lack of a drug effect during the study period, whereas the graph to the far right would suggest that the drug either acted as a sensitizer to an underlying defect or even caused disease.

Possible Disease/Drug Interaction Curves
Reproduced with permission from F Gorelick, MD.
In closing, Dr. Gorelick's supported the need for long-term prospective studies to identify the risk/benefit for the GLP-1 agonists, but in the meantime he believes the data from animal and human studies call for vigilance, regular data examination, and continued open discussion.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.