

Summary
Emergency percutaneous coronary intervention (PCI) of an infarcted coronary artery is an efficacious treatment for patients with acute ST-segment elevation myocardial infarction (STEMI). However, the value of performing PCI on these arteries (preventive PCI) during primary PCI for STEMI is unknown. The objective of the Preventive Angioplasty in Myocardial Infarction trial [PRAMI; Wald DS et al. N Engl J Med 2013] was to determine whether preventive PCI performed during the same procedure as the infarct-artery PCI would reduce the incidence of cardiac-related death, nonfatal MI, or refractory angina with evidence of ischemia.
- Interventional Techniques & Devices Cardiology Clinical Trials
- Myocardial Infarction
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
- Myocardial Infarction
Emergency percutaneous coronary intervention (PCI) of an infarcted coronary artery is an efficacious treatment for patients with acute ST-segment elevation myocardial infarction (STEMI). Patients presenting with STEMI commonly also have other, noninfarct-artery major stenoses. However, the value of performing PCI on these arteries (preventive PCI) during primary PCI for STEMI is unknown. Based on a lack of evidence for preventive PCI in patients with stable coronary artery disease, cardiovascular guidelines recommend against such practice. The objective of the Preventive Angioplasty in Myocardial Infarction trial [PRAMI; Wald DS et al. N Engl J Med 2013], presented by David S. Wald, MD, Barts and the London Medical School, London, United Kingdom, was to determine whether preventive PCI performed during the same procedure as the infarctartery PCI would reduce the incidence of cardiac-related death, nonfatal MI, or refractory angina with evidence of ischemia.
A total of 465 consecutive patients with acute STEMI and multivessel coronary disease detected at the time of emergency PCI of the infarct artery were enrolled in this randomized, multicenter, single-blind study between 2008 and 2013. Multivessel disease was defined as >50% stenosis in one or more noninfarct arteries suitable for PCI. Ineligible patients included those with cardiogenic shock, prior coronary artery bypass graft surgery, >50% stenosis in either the left main or ostia of both the left anterior descending and circumflex arteries or if the only noninfarct stenosis was a chronic total occlusion. The patients were randomized after successful emergency PCI to preventive PCI (n=234) or no preventive PCI (n=231) in the noninfarct artery while they were still in the catheterization laboratory. The patients were examined and evaluated with electrocardiography at 6 weeks and annually thereafter.
Baseline characteristics were similar between the two groups. The mean age in both groups was 62 years, 76% were male, and the majority of infarcts involved the inferior wall, with approximately one-third anterior infarcts. The trial was stopped on January 24, 2013, due to a highly significant difference in the primary outcome in favor of preventive PCI (p<0.001).
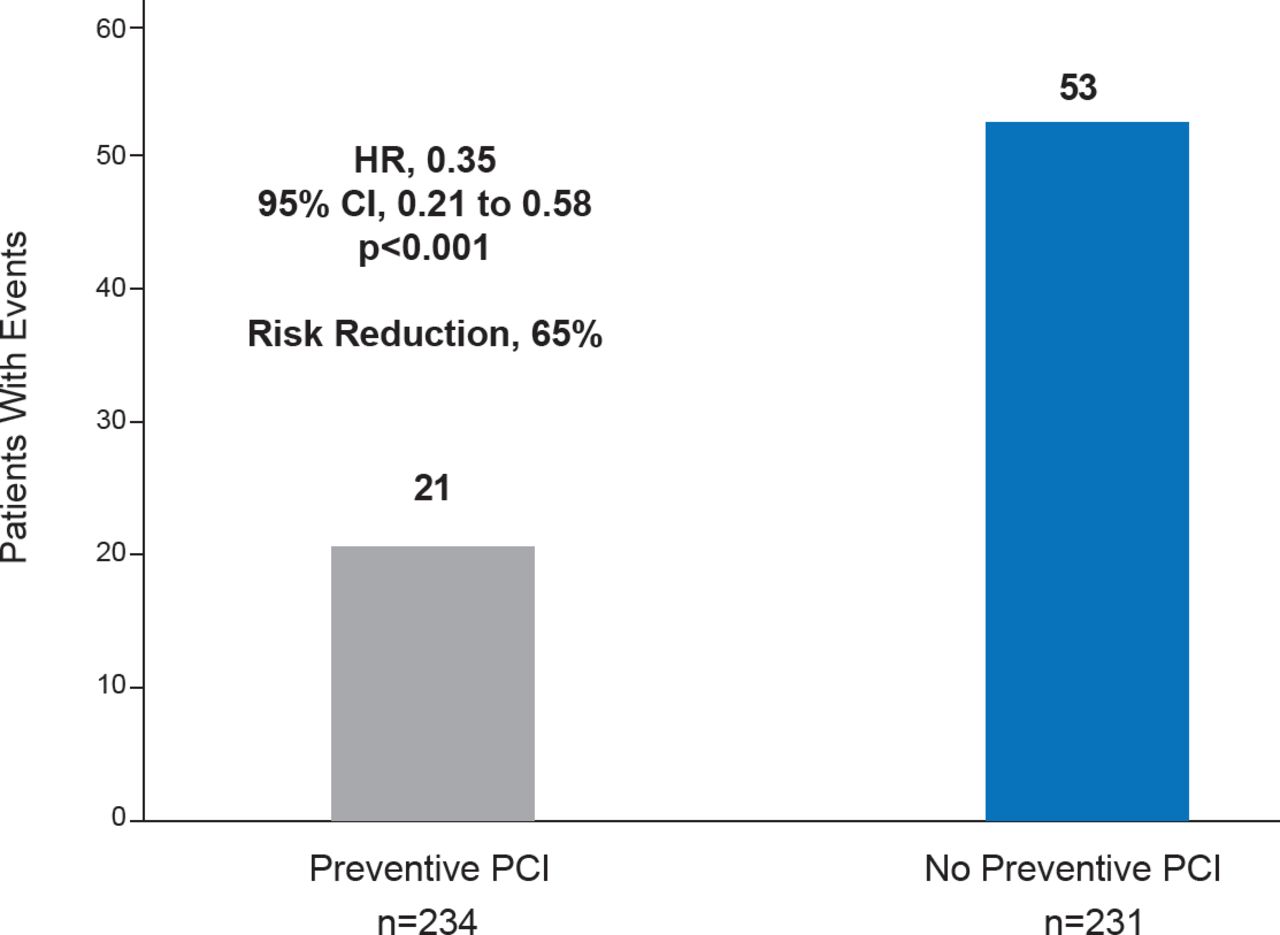
The mean follow-up was 23 months. Ten patients in the preventive PCI group and 8 in the no preventive PCI group were lost to follow-up. The primary composite outcome occurred in 21 patients in the preventive PCI group (9.0%) and 53 patients in the no preventive PCI group (22.9%), with a risk reduction of 65% in the preventive PCI group (HR, 0.35; 95% CI, 0.21 to 0.58; p<0.001; Figure 1). This translates into an absolute risk reduction of ∼14% or a number needed to treat of 7 patients to prevent one primary endpoint event at 1 year.

Cardiac Death, Nonfatal MI or Refractory Angina
Reproduced with permission from DS Wald, MD.
Cardiac death or nonfatal MI occurred in 11 (4.7%) patients in the preventive PCI group and 27 (11.7%) patients in the no preventive PCI group, with a risk reduction of 64% for patients treated with preventive PCI (HR, 0.36; 95% CI, 0.18 to 0.73; p=0.004). This translates into an absolute risk reduction of ∼7% or a number needed to treat of 15 patients to prevent one cardiac death or nonfatal MI at 1 year.
Procedure-related complications occurred in 10 patients in the preventive PCI group and 9 patients in the no preventive PCI group, and were composed of contrast nephropathy, bleeding requiring transfusion or surgery, and stroke. However, the trial was not powered to adequately compare the safety of these two strategies.
The results of the PRAMI trial demonstrate that preventive PCI performed in noninfarct arteries immediately after emergency PCI for STEMI provides a substantial cardiac benefit at 1 year. The robust results of this preventive PCI trial in the context of primary STEMI care are counter to current standards of care. Previously, due to uncertainty of the value of preventive PCI, its practice varied among cardiologists. It will be interesting to see whether the next iterations of major cardiovascular guidelines adopt the results of this trial.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.