

Summary
This article discusses guideline management of acute coronary syndromes (ACS), including ST elevation myocardial infarction (NSTEMI), ST-elevated myocardial infarction (STEMI), and management after ACS.
- Myocardial Infarction
- Myocardial Infarction
- Cardiology
Maarten L. Simoons, MD, Thoraxcenter, Erasmus University Medical Center, Rotterdam, The Netherlands, discussed guideline management of acute coronary syndromes (ACS).
STEMI MANAGEMENT
ACS is a spectrum of pathophysiological conditions that includes unstable angina (UA), non-ST elevation myocardial infarction (NSTEMI) and ST-elevated myocardial infarction (STEMI). The classification of the type of ACS involves measuring biomarkers of cardiac myocyte necrosis (preferably troponin T or I or, if these are not available, creatine kinase-MB). Patients with UA present with angina (either accelerating in nature or at rest) but have no rise in cardiac biomarkers. Patients with angina and elevated cardiac biomarkers have an MI and are further classified as either NSTEMI or STEMI based upon an electrocardiogram (ECG).
The increased sensitivity of the assays used to measure necrosis has made it possible to detect very small amounts of myocardial necrosis. These enhanced detection techniques have led to an evolving definition of an MI. Under the current Universal Definition of Myocardial Infarction (2012), an MI is confirmed when there is evidence of myocardial necrosis—identified by a rise and fall of necrosis markers (preferably troponin)—with at least one value >99% of the upper reference limit in a clinical setting of symptomatic or image-verified myocardial ischemia [Thygesen K et al. Eur Heart J 2012].
This universal definition recognizes several types of MI. The primary MI, or Type 1 MI, includes plaque rupture leading to intracoronary thrombus. In Type 2, the cause of the MI is an imbalance of oxygen supply and demand in the myocardium caused by arrhythmia, hypertrophic cardiomyopathy, severe anemia, or cardiogenic, hypovolemic, or septic shock. Type 3 MIs are characterized as cardiac death with symptoms suggestive of MI, or ST changes in the ECG or left bundle branch block in a patient for whom biomarker values are not available. Type 4 or 5 MIs are those associated with percutaneous coronary intervention or coronary artery bypass graft, respectively. Myocardial necrosis may also result from injury that is not related to myocardial ischemia (eg, trauma, cardiotoxic agents, myocarditis) and/or other undetermined myocardial injury (eg, heart failure, pulmonary embolism, etc) [Thygesen K et al. Eur Heart J 2012].
Early diagnosis is critical and may be achieved via onsite ECG interpretation by computer, by the ambulance staff or by phone transmission of the ECG to the hospital. Relief of chest pain and dyspnea, ECG monitoring, and immediate reperfusion therapy should follow. Prof. Simoons stressed that immediate reperfusion therapy in acute MI reduces infarct size and increases hospital as well as long-term survival [Boersma E et al. Lancet 1996]. It is also associated with lifelong benefits, with one study reporting a gain of ∼3 years in life-expectancy [Domburg RT et al. Eur J Prev Cardiol 2012].
The consistent delivery of early reperfusion therapy requires public awareness of MI symptoms, rapid response by physicians and ambulances to emergency calls, prehospital diagnosis (ECG), and regional arrangements to avoid delays. Prof. Simoons described the REPAIR Program (Reperfusion Acute Infarction Rotterdam) that has been in place since 1988. This program coordinates STEMI management for all of the hospitals in Rotterdam. Under this system, patients with a STEMI are either transported to one of two centers that are able to provide immediate reperfusion services (Thoraxcenter, Erasmus MC, or Maasstad ziekenhuis). If the patient does not appear to be having an infarction based upon the initial triage, they are sent to another Rotterdam hospital for observation.
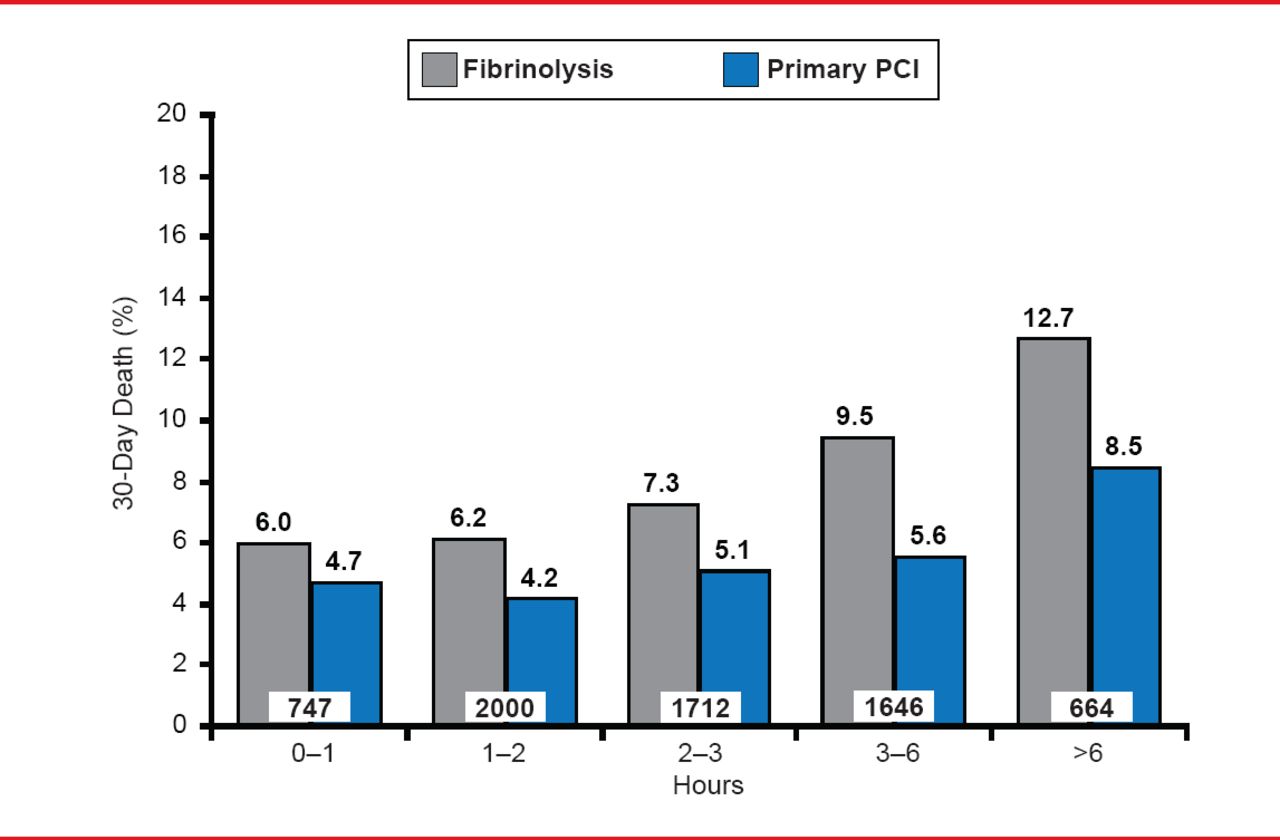
For STEMI patients, the optimal lifesaving strategy entails primary PCI plus stenting by an experienced team within 90 to 120 minutes after initial medical contact. If that is not possible, fibrinolytic therapy (fibrin-specific agent) should be started, preferably in an ambulance (Figure 1) [Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology. Eur Heart J 2012].

30-Day Death Rate: Fibrinolysis Versus Primary PCI in STEMI Patients
Reproduced from Boersma E et al. Does time matter? A pooled analysis of randomized clinical trials comparing primary percutaneous coronary intervention and in-hospital fibrinolysis in acute myocardial infarction patients. Eur Heart J 2006;27(7):779–788. With permission from Oxford University Press.
Patients who qualify for fibrinolytic therapy should receive either alteplase or tenecteplase, combined with aspirin 150 to 300 mg oral/IV. Clopidogrel 300 mg should also be given since ticagrelor and prasugrel have not been tested for use with fibrinolysis. Anticoagulation therapy (preferably with enoxaparin) is recommended until revascularization. While there are contraindications for fibrinolytic therapy, all patients should continue to receive medical therapy in accordance with current guidelines.
MANAGEMENT OF NSTEMI
Patients with NSTEMI should be admitted to a chest-pain or cardiac care unit for an ECG with either ST monitoring or repeated 12-lead ECG. In addition, the risk of cardiac events and bleeding should also be assessed for each individual. Troponin (I/T) should be measured at admission, after 6 to 9 hours, and in some patients again after 12 to 24 hours. An ECG is also appropriate at some point to assess left ventricular function.
Initial management of patients with NSTEMI should include antithrombotic therapy with unfractionated heparin and dual antiplatelet therapy with aspirin and either ticagrelor, prasugrel, or clopidogrel. Anti-ischemic therapy with β-blockers or nitrates should be utilized as appropriate. An invasive strategy may be considered to prevent recurrent ischemia and improve prognosis for patients with ACS, particularly in those with recurrent ischemia, major arrhythmia, hemodynamic instability, and multiple high-risk characteristics.
MANAGEMENT AFTER ACS
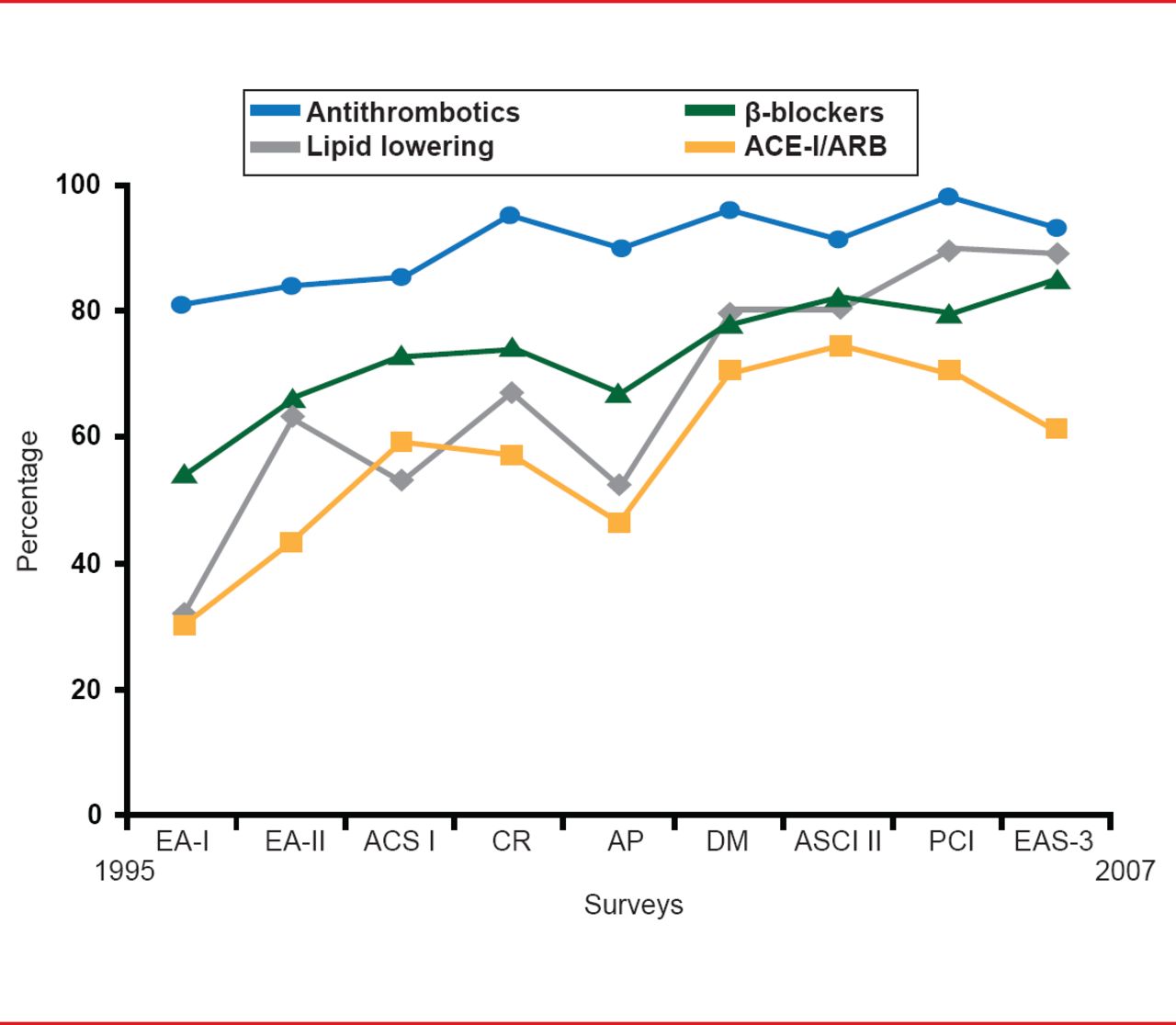
Preventive medical therapy after ACS includes the initiation of statins as soon as possible; β-blockers as soon as the patient is stable. Patients with left ventricular ejection fraction ≤40% also benefit from initiation of an angiotensin-converting enzyme (ACE) inhibitor (or angiotensin receptor blockers if ACE inhibition is not tolerated). Dual antiplatelet therapy with aspirin and clopidogrel/prasugrel/ticagrelor should be continued for 1 year (Figure 2). Lifestyle interventions include smoking cessation, weight control, and exercise. Patients should be assessed for diabetes and hypertension, and treated as necessary.

Management After ACS
ACE-I=angiotensin-converting enzyme inhibitor; ARB= angiotensin receptor blockers.
Source: Euro Heart Survey Programme ESC Report: Cardiovascular Disease in Europe 2006.
In summary, the important components of an ACS management program include
-
▪ Early recognition of symptoms by the patient
-
▪ Prehospital diagnosis if possible (ambulances with ECG interpretation)
-
▪ Immediate reperfusion in STEMI (PCI or fibrinolytic)
-
▪ Intensive medical therapy
-
» Antithrombotic, statin, β-blocker, ACE-inhibition
-
» Revascularization in high-risk patients
-
-
▪ Secondary prevention
-
» Abstaining from smoking in particular
-
» Appropriate food, exercise
-
» Management of hypertension and diabetes if present
-
» Antithrombotics, statin, β-blocker, ACE-inhibition
-
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.