

Summary
Since pregnancy induces major changes in maternal thyroid function, management of thyroid diseases at this time requires special care to prevent adverse effects on the pregnancy and developing fetus. This article discusses how challenging this can be in the absence of unified clinical practice guidelines.
- Thyroid Disorders
- Pregnancy
- Thyroid Disorders
- Endocrinology
- Diabetes & Metabolic Syndrome
- Pregnancy
Since pregnancy induces major changes in maternal thyroid function, management of thyroid diseases at this time requires special care to prevent adverse effects on the pregnancy and developing fetus. Alex Stagnaro-Green, MD, George Washington University, Washington, DC, USA, discussed how challenging this can be in the absence of unified clinical practice guidelines.
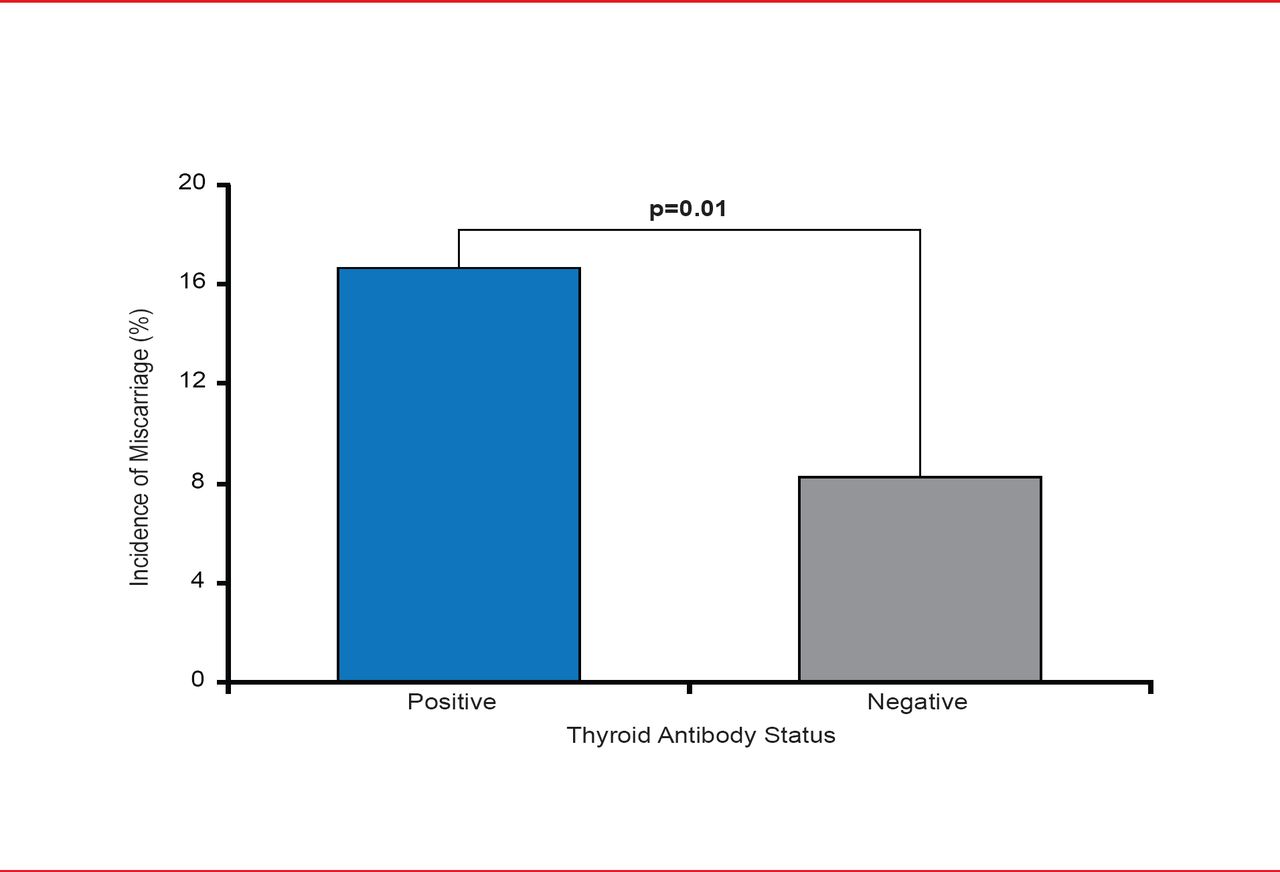
In the last 2 decades, there have been rapid advances in knowledge regarding thyroid dysfunction during pregnancy. Studies have reported a doubling of the miscarriage rate in antibody positive (Ab+) euthyroid women (Figure 1) [Stagnaro-Green A et al. JAMA 1990], as well as an increase in preterm delivery [Ghafoor F et al. J Coll Physicians Surg Park 2006; Negro R et al. J Clin Endocrinol Metab 2006; Gilnoer D et al. J Clin Endocrinol Metab 1991].

The Relationship Between Miscarriage Rate and Thyroid Antibody Status
Source: Stagnaro-Green A et al. JAMA 1990.
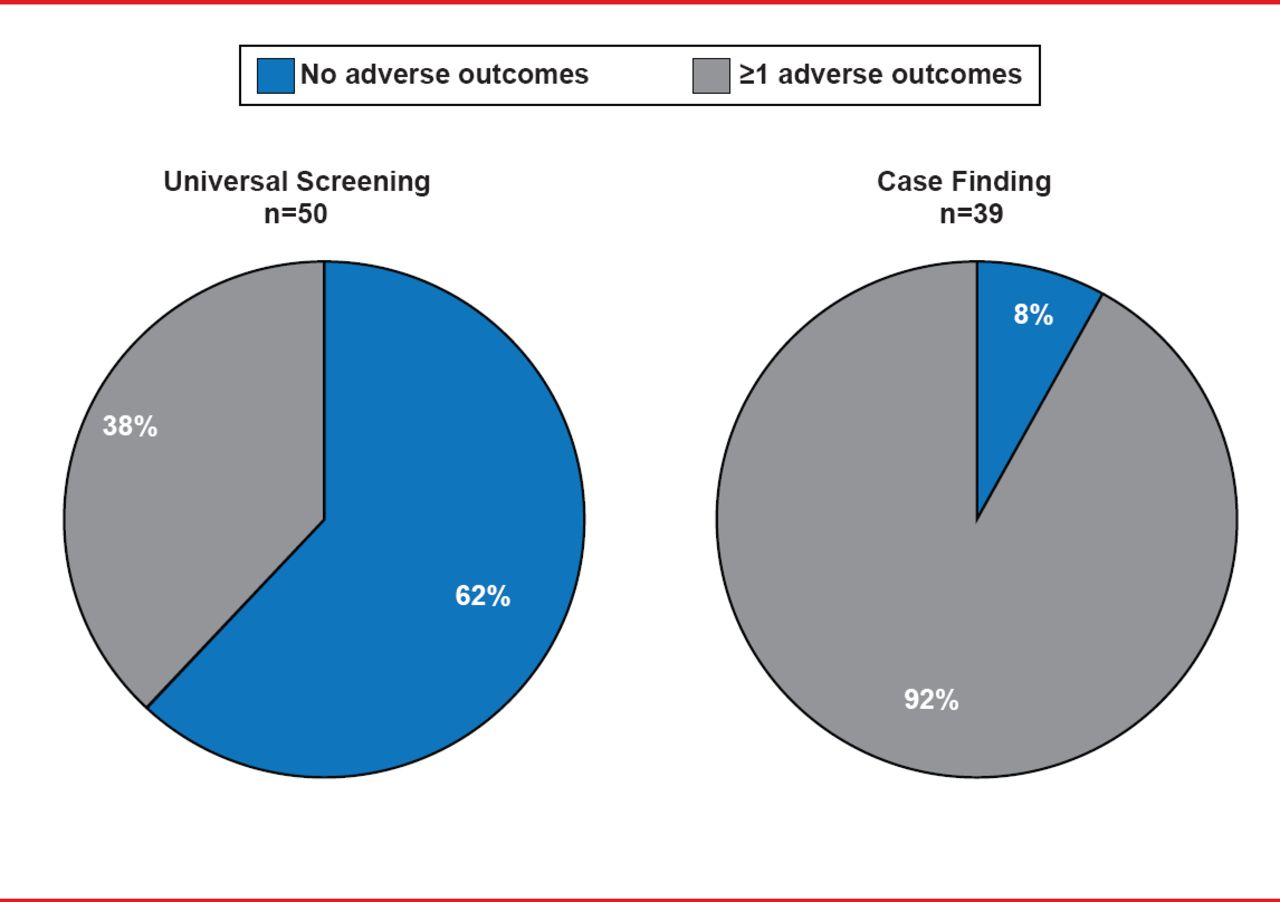
Subclinical hypothyroidism (SCH), reported to occur in up to 15.5% of all pregnant women [Blatt AJ et al. J Clin Endocrinol Metab 2012], has also been shown to be associated with increased rates of miscarriage or fetal death [Ashoor G et al. Thyroid 2010], and preterm delivery [Casey BM et al. Obstet Gynecol 2005]. Although only 1 study has investigated the impact of treating maternal SCH on maternal and fetal complications, the findings were striking. In women who had universal screenings for thyroid disease early in pregnancy, 62% had no adverse obstetrical or neonatal outcomes [Negro R et al. J Clin Endocrinol Metab 2010]. However, in women who were not identified as hypothyroid until postpartum, only 8% had no adverse findings (Figure 2).
Despite the abundance of new clinical information that has emerged in recent decades, controversy still exists in relation to recommendations for detection and management of thyroid disease during pregnancy, with continued debate between the American College of Obstetrics and Gynecology (ACOG), The Endocrine Society (TES), and the American Thyroid Association (ATA).
For example, ACOG does not recommend treatment of SCH, while TES recommends treatment with levothyroxine in women who are positive or negative for thyroid antibodies. The ATA recommends treating SCH in antibody positive women, but considers the data insufficient to recommend for or against treating SCH during pregnancy in women with a thyroid-stimulating hormone between 2.5 and 10.0 who are antibody negative.

Outcomes Associated With Treating Hypothyroid Pregnant Women
Souce: Negro R et al. J Clin Endocinol Metab 2010.
Additionally, both the ATA and TES recommend screening for thyroid disease in all groups who have an increased risk for thyroid disease. In fact, a subgroup of the members who created guidelines for TES recommended screening all pregnant women for thyroid disease. On the other hand, ACOG recommends screening only a small subgroup of pregnant women.
Although universal guidelines for management of thyroid disease during pregnancy would provide clarity for patients and clinicians, according to Dr. Stagnaro-Green, there are numerous barriers to their establishment. Perceptions vary between the different organizations regarding the importance of the topic, and each has a different philosophy on granularity according to its focus. Additionally, organizations interpret data variably, and differ in their ideas on how much data are needed to produce a guideline. He remarked that although a consensus opinion is unlikely due to the difference in granularity of guidelines and interpretation of data between ACOG and the other two societies, the outcome of future studies might provide some impetus for these organizations to work together to produce consensus guidelines for clinicians and patients.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.