

Summary
Biomarkers are important diagnostic tools that help physicians determine a patient's risk for developing a disease and can guide clinical decisions. However, at times, it is critical to understand if a specific biomarker causes disease or is merely reflective of the disease process. This distinction is important mainly if the biomarker is intended to be a therapeutic target (ie, lowering a biomarker with a drug with the hopes of lowering risk for disease). In humans, randomized controlled clinical trials and human genetics are two approaches to understand causal factors. This article discusses a human genetics approach—Mendelian randomization—to distinguish causal from noncausal biomarkers.
- Myocardial Infarction
- Cardiology Genomics
- Lipid Disorders
- Hematology
- Myocardial Infarction
- Cardiology Genomics
- Lipid Disorders
Biomarkers are important diagnostic tools that help physicians determine a patient's risk for developing a disease and can guide clinical decisions. However, at times, it is critical to understand if a specific biomarker causes disease or is merely reflective of the disease process. This distinction is important mainly if the biomarker is intended to be a therapeutic target (ie, lowering a biomarker with a drug with the hopes of lowering risk for disease). In humans, randomized controlled clinical trials and human genetics are two approaches to understand causal factors. Sekar Kathiresan, MD, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts, USA, discussed a human genetics approach—Mendelian randomization—to distinguish causal from noncausal biomarkers and presented the question, “Which lipid pathways have a causal relationship for myocardial infarction?”
The leading cause of death in the world, myocardial infarction (MI), is a heritable condition [Roger VL. Circulation 2012]. In the United States, 610,000 new MIs occur each year. Observational epidemiology studies provided the initial clues behind the mechanisms that cause MI. In the original Framingham Study that was published in 1961, increasing serum cholesterol levels were associated with increasing incidence rate per 1000 individuals [Kannel WB et al. Ann Int Med 1961]. Since then, research has advanced the understanding of the structure and function of lipoproteins, including the presence of high-density lipoproteins (HDL), low-density lipoproteins (LDL), and the lowest density lipoproteins—very LDL and chylomicrons.
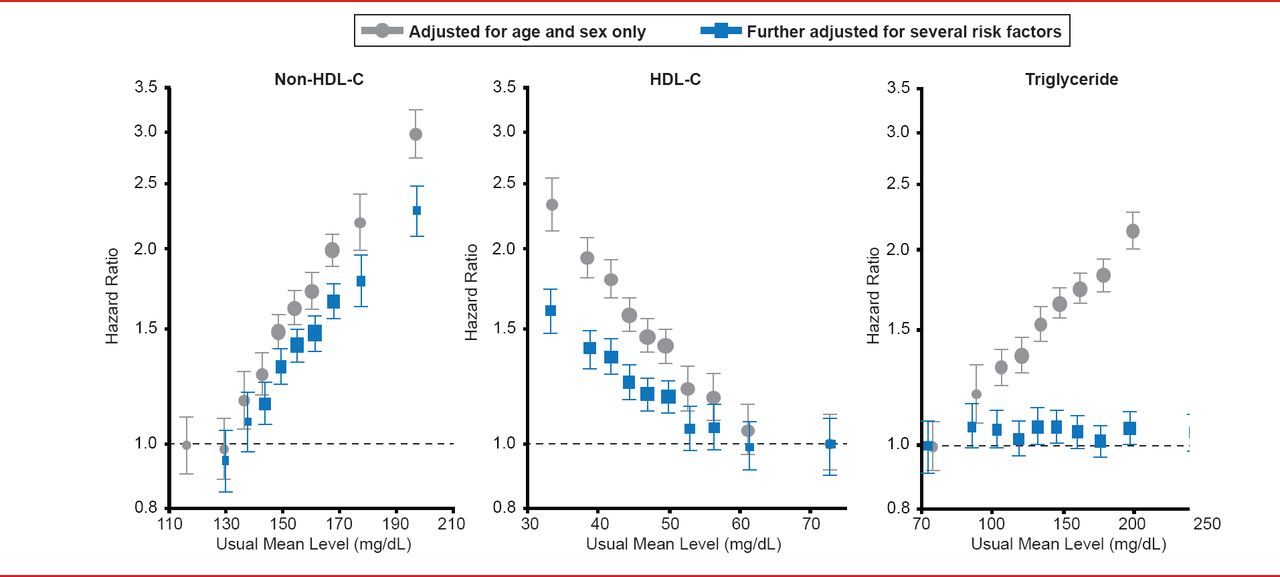
In a more recent study, the mean serum levels of LDL, HDL, and triglyceride serum levels were plotted against the hazard ratio (HR) for risk of coronary heart disease (CHD) [The Emerging Risk Factors Collaboration. JAMA 2009]. Increasing levels of LDL were associated with an increased HR, whereas increasing HDL levels were associated with decreased HR (Figure 1). Although increasing triglyceride levels appear to be associated with increased HR, when the data were adjusted for other risk factors, the relationship disappeared. Dr. Kathiresan stated that based on the information about LDL, HDL, and triglycerides, HDL was viewed as the “key protective factor” in CHD, while the role of triglycerides is less clear.

Lipoprotein Association With Risk of CHD
Reproduced from The Emerging Risk Factors Collaboration. Major Lipids, Apolipoproteins, and Risk of Vascular Disease. J JAMA 2009;302(18):1993–2000. With permission from the American Medical Association.
Dr. Kathiresan said that a causal relationship is difficult to establish based on observational epidemiology. For example, a soluble biomarker such as HDL may be demonstrated in the literature to be associated with a disease, such as MI. However, the same relationship could be demonstrated if reverse causation—the disease process itself increases the soluble biomarker—were true, or if a confounder was present. Epidemiological studies are not able to distinguish between causation, reverse causation, and confounders. One way to demonstrate true causality is by a randomized, controlled trial; however, it would be time consuming and expensive to do this for every potential biomarker.
A second potential way to demonstrate causality is by human genetics through Mendelian randomization (Figure 2) [Hingorani A, Humphries S. Lancet 2005]. The theory behind Mendelian randomization is that the random allocation of alleles during meiosis is similar to the randomization performed in a randomized, controlled trial. Several advantages of Mendelian randomization are that genotypes are not modified by disease, thereby minimizing reverse causation, and genotypes are randomly assigned during meiosis, which minimizes confounding factors.

Comparison of a Randomized, Controlled Trial to Mendelian Randomization
CV=cardiovascular.
Reproduced from Hingorani A, Humphries S. Nature's randomised trials. Lancet 2005;366(9501):1906–1908. With permission from Elsevier.
To evaluate a potential biomarker using Mendelian randomization, the gene variants, called “instruments,” that code for the biomarker of interest are used to develop a theoretically predicted risk estimate, which is based on the amount of change in the biomarker from baseline and how that extent of biomarker change is expected to affect disease risk in a population. As a result, a disease risk can be estimated. Then, the variant can be directly associated with disease in the population and this observed risk estimate can be compared with that theoretically predicted. If the observed risk estimate matches that theoretically predicted, this would lend support to the idea that the biomarker is causal for the disease.
To illustrate Mendelian randomization in MI, Dr. Kathiresan used the example of LDL cholesterol as a causal biomarker for MI. A variant of the gene PCSK9 was found in 3.2% of individuals, which resulted in a 15% decrease in serum LDL levels and a 45% decrease in CHD risk compared with individuals with wild-type PCSK9 [Cohen JC et al. N Engl J Med 2006]. The gene variant is PCSK9, the biomarker is circulating LDL cholesterol levels, and the disease is CHD risk. The observed risk is the relative risk for CHD in individuals who are carriers for the PCSK9 variant compared with individuals with wild-type PCSK9 (Figure 3). Based on the fact that the PCSK9 variant led to a 21-mg/dL decrease in serum LDL cholesterol, one would expect carriers of this mutation to be protected from risk for CHD by 20% (theoretically predicted risk estimate OR 0.80 (range, 0.78 to 0.83). When the PCSK9 variant was directly tested for association with CHD in the population, the observed risk estimate was 28% decrease in risk for CHD. Here, as the observed risk estimate matched the theoretically predicted, Dr. Kathiresan stated these data indicate that LDL is a causal factor of CHD and suggested that inhibition of PCSK9 could lower CHD risk.

Schematic of Mendelian Randomization for the LDL Biomarker
CHD=coronary heart disease; LDL-C=low-density lipoprotein cholesterol; MI=myocardial infarction.
Reproduced with permission from S Kathiresan, MD.
Several companies have begun development of PCSK9 inhibitors, primarily through monoclonal antibodies. In Phase 2 trials, PCSK9 monoclonal antibody injections in combination with statins result in about a 50% decrease in serum LDL cholesterol levels [Stein EA et al. N Engl J Med 2012; Dias CS et al. J Am Coll Cardiol 2012]. Phase 3 trials evaluating the efficacy of PCSK9 inhibitors on CHD risk are currently underway.
For HDL cholesterol as a biomarker for CHD, a recent case-control trial evaluated a variant of LIPG, which causes serum HDL cholesterol levels to be elevated in carriers [Voight BF et al. Lancet 2012]. The variant is present in −3% of individuals and results in a 6-mg/dL increase in serum HDL cholesterol. Therefore, it would be expected that carriers of the LIPG variant would have a relative risk ratio of 0.87 (range, 0.84 to 0.91) for CHD. However, in this study of 116,320 individuals, carriers of the LIPG variant did not have a lower risk for CHD. In this study, the relative risk was 0.99 (range, 0.88 to 1.11; p=0.80). In addition, individuals with a combination of single nucleotide polymorphisms (SNPs) that raise serum HDL cholesterol also did not demonstrate a decrease in MI risk [Voight BF et al. Lancet 2012]. Dr. Kathiresan suggested that an intervention that raises serum HDL level cannot be assumed to lead to a lower risk for MI.
A randomized, controlled trial evaluated dalcetrapib in about 16,000 patients was halted early for futility. Although dalcetrapib raised serum HDL cholesterol by −30%, it did not result in a decreased risk for MI [dal-OUTCOMES; Schwartz GG et al. N Engl J Med 2012]. Dr. Kathiresan suggested that the reason low serum HDL cholesterol level is associated with increased MI risk is because low HDL tracks with multiple other confounding factors that are also associated with MI.
Mendelian randomization for serum triglyceride levels is more challenging than LDL and HDL, because a gene variant that affects serum triglyceride levels also affects other traits that may be important in MI. Using a novel analytical method, Dr. Kathiresan's research group has generated data that suggest that triglyceride-rich lipoproteins most likely are causal factors in CAD. He went onto describe three specific genes that alter plasma triglycerides and affect risk for CAD—lipoprotein lipase, apolipoprotein A5, and apolipoprotein C3.
Although traditional epidemiology can provide clues about factors that may have a causal link to a disease process, it cannot provide a definitive answer. Although randomized, controlled trials are the gold standard to establish causation, it is a challenging approach in the identification of biomarkers. Instead, Mendelian randomization appears to be a promising new approach that can accurately identify biomarkers that have a causal relationship in a disease process.

MANY THANKS The editors would like to thank the many members of the XXIV Congress of the ISTH presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.