

Summary
Cardiac resynchronization therapy (CRT) continues to benefit many patients with heart failure (HF), reducing their symptoms and enhancing clinical outcomes and quality of life. This article discusses a series of sessions which covered current perspectives on CRT, including techniques to approach the left ventricle (LV) and optimize lead placement, as well as data from clinical trials that favor the use of triventricular (TriV) pacing. Specific topics include device implantation and optimal lead placement, improving CRT response and optimizing LV site positioning, and the the Dual-Site LV Pacing in CRT Non Responders: Multicenter Randomized Trial [V3; NCT01059175; Bordachar P et al. J Card Fail 2010].
- Heart Failure
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Heart Failure
- Interventional Techniques & Devices
Cardiac resynchronization therapy (CRT) continues to benefit many patients with heart failure (HF), reducing their symptoms and enhancing clinical outcomes and quality of life. Jean-Luc Jansens, MD, University of Brussels, Brussels, Belgium, launched a series of sessions which covered current perspectives on CRT, including techniques to approach the left ventricle (LV) and optimize lead placement, as well as data from clinical trials that favor the use of triventricular (TriV) pacing.
DEVICE IMPLANTATION AND OPTIMAL LEAD PLACEMENT
Historically, attention has been placed on the technical aspects of the procedure, especially LV lead placement which is pivotal for optimal cardiac synchronization. The gold standard technique for device implantation remains the percutaneous approach. However, its disadvantages include implantation failure and inadequate lead positioning, and reliance on the venous anatomy of the heart, which differs between patients.
Surgery is typically viewed as a back-up procedure for CRT device implantation in cases of percutaneous failure. However, Prof. Jansens remarked that it should also be considered for its ability to improve the CRT response. Robotic surgery in particular is used to optimize LV lead positioning, and implant LV leads for multisite pacing.
Various surgical approaches are used for CRT device implantation:
-
▪ Thoracotomy is technically easy, but optimum lead placement is problematic due to difficulty exposing the entire LV
-
▪ Conventional thoracoscopy improves LV exposure, but requires the use of rigid tools to suture a lead onto the beating heart
-
▪ Robotic enhanced thoracoscopy offers improved surgical precision, and is minimally traumatic. However, equipment is expensive, and the learning curve is steep
IMPROVING CRT RESPONSE AND OPTIMIZING LEFT VENTRICLE SITE POSITIONING
Although epicardial leads have a poor reputation in the cardiosurgical field, there is no major evidence against their long-term efficiency. Prof. Jansens noted that they often produce better results than endocardial leads, and in his opinion, steroid-eluting tips represent the best option for epicardial lead implantation.
Yet, despite the success of CRT, the nonresponder rate is >30%, and has remained unchanged for many years [Yu CM et al. J Cardiovasc Electrophysiol 2005]. Since suboptimal LV lead implantation is an important reason for this, effort must be made to improve its positioning, using cardiosurgical tools to facilitate hemodynamic and electroanatomic mapping.
Conventionally, biventricular (BiV) pacing is achieved using one right atrial (RA) lead and one right ventricular (RV) lead, and the LV lead for epicardial pacing is implanted into the coronary sinus. However, we know that LV dyssynchrony typically involves a large area of the heart, so pacing in one epicardial spot may not completely correct dyssynchrony.
Multisite pacing of the LV is therefore an option for nonresponders to conventional CRT. Christophe Leclercq, MD, PhD, Rennes University Hospital, Rennes, France, discussed the rationale behind this. Since BiV pacing can result in suboptimal resynchronization, leading to inadequate or no response to CRT, his team designed a clinical trial to compare the effects of TriV with BiV pacing, the Triple Resynchronization in Paced Heart Failure Patients trial [TRIP-HF; Leclercq C et al. J Am Coll Cardiol 2008].
This multicenter study enrolled 40 patients (mean age, 70 years) with moderate to severe HF, and a mean LV ejection fraction (LVEF) of 26%. All patients were in permanent atrial fibrillation.
After 3 months of BiV stimulation, patients were randomized to stimulation for 3 months with TriV pacing or conventional BiV pacing. Patients were then crossed over to the alternate configuration for a further 3 months. The primary endpoint of the study was quality of ventricular resynchronization (Z ratio). Secondary endpoints included reverse LV remodeling [Leclerq C et al. J Am Coll Cardiol 2008].
A significantly increased LVEF (27% vs 35%; p=0.001), decreased LV end-systolic volume (157 vs 134 cm3; p=0.02), and decreased diameter (57 vs 54 mm; p=0.02) were seen with TriV pacing than with BiV pacing, and the investigators concluded that CRT using TriV pacing was safe, and associated with significantly more LV reverse remodeling than with BiV pacing.
Prof. Leclercq then discussed recently published data from the Efficiency Study of Triple-Site Cardiac Resynchronization in Patients With Heart Failure [TRUST CRT; NCT00814840; Lenarczyk R et al. J Cardiovasc Electrophysiol 2012].
TRUST CRT was a single-center, prospective study designed to assess implantation feasibility and safety, procedure-related adverse events and lead performance for 12 months in patients included in a trial of CRT using TriV pacing. It enrolled 100 patients (mean age 62 years; 79% male; 61% with ischemic cardiomyopathy; 86% in NYHA Functional Class III) who were randomized to CRT with BiV or TriV pacing.
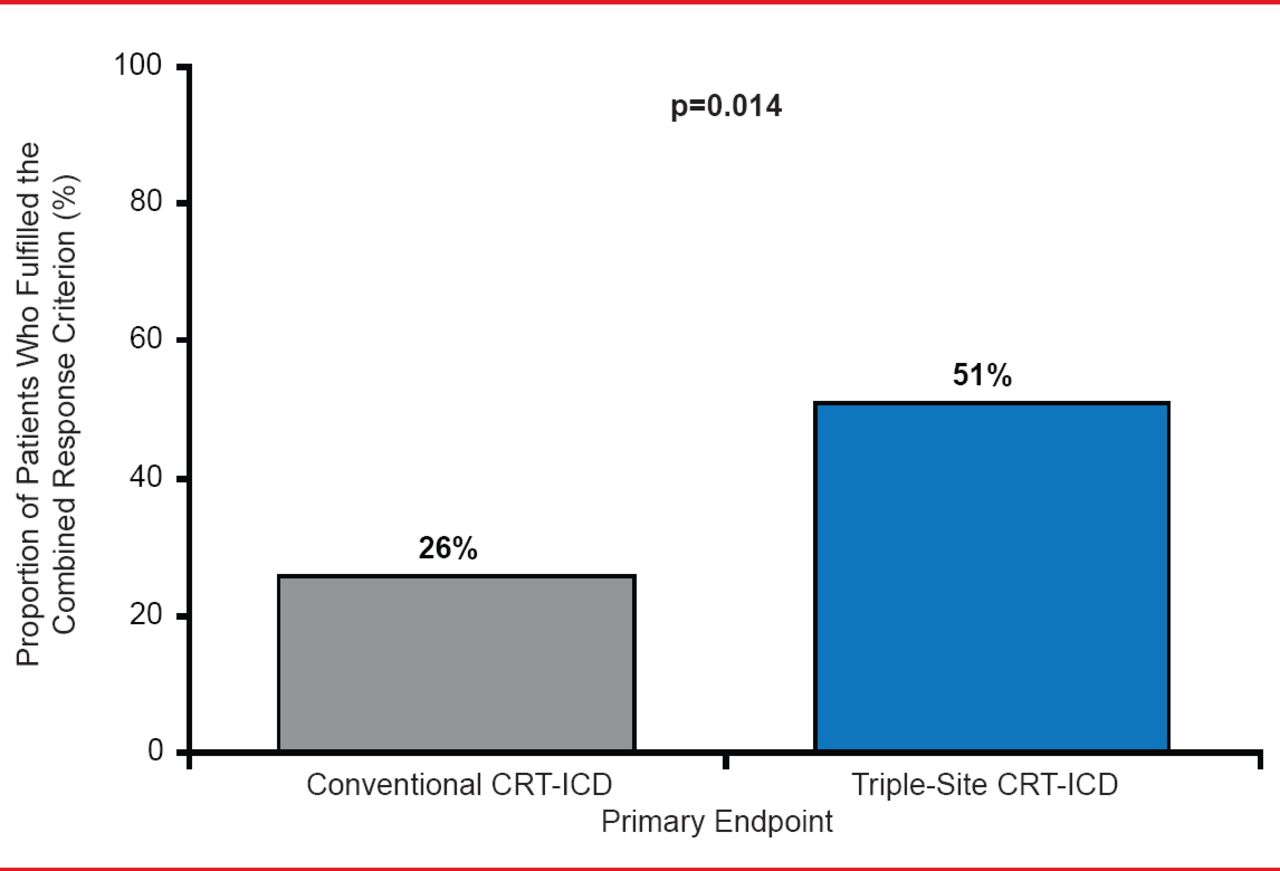
Primary endpoints included the combined endpoint of alive status, and freedom from hospitalization for HF or heart transplantation. A significant improvement in the rate of responders was seen in the TriV pacing group compared with the BiV pacing group (51% vs 26%; p=0.014; Figure 1) [Lenarczyk R et al. J Cardiovasc Electrophysiol 2012].

Rate of Responders
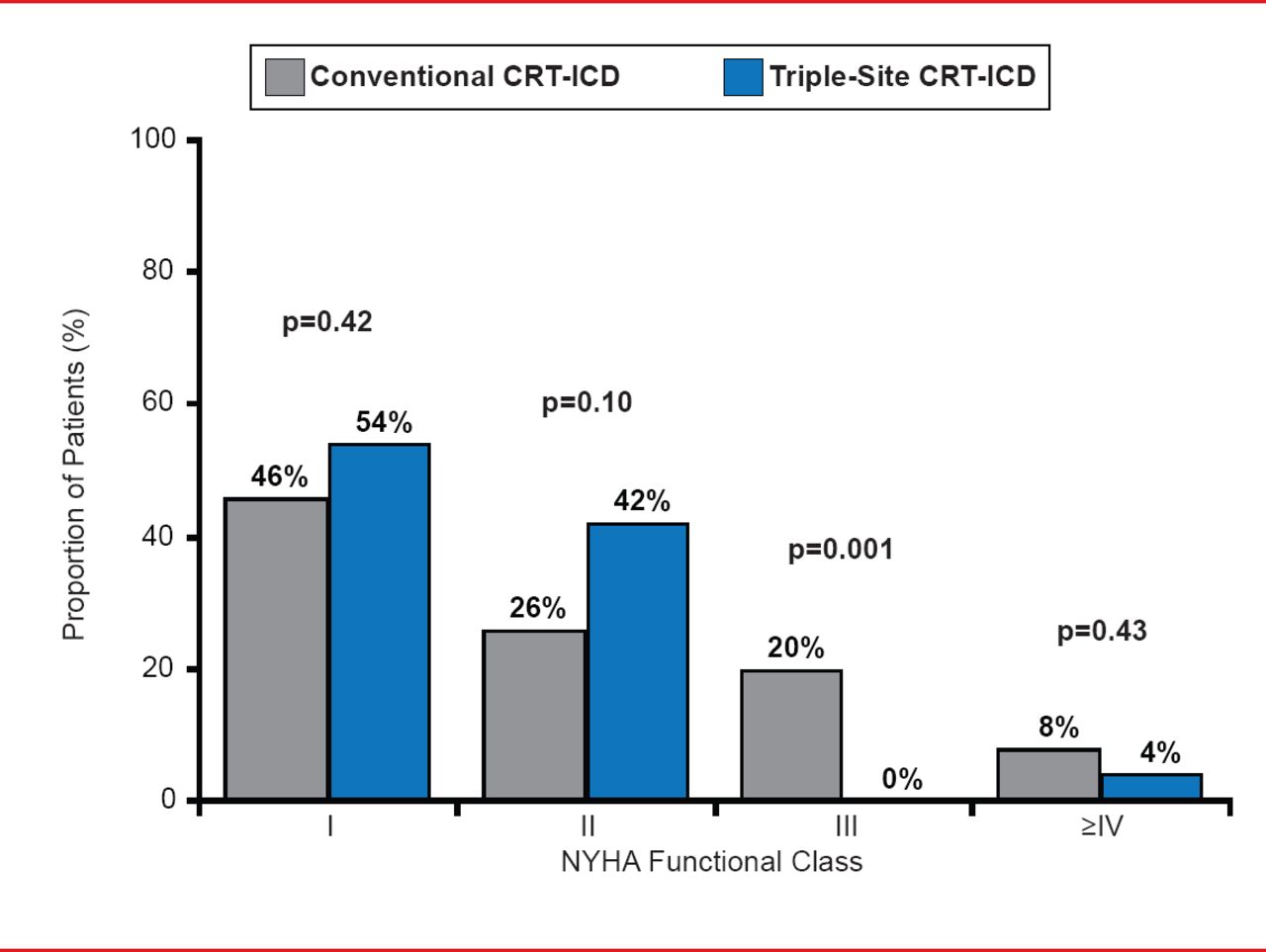
And after 12 months, significantly more patients with BiV pacing were in NYHA Functional Class III or IV than those with TriV pacing (30% vs 12.5%; p=0.05; Figure 2).

NYHA Functional Classification
Adapted from Lenarczyk R et al. J Cardiovasc Electrophysiol 2013.
Finally, Prof. Leclercq discussed the Dual-Site LV Pacing in CRT Non Responders: Multicenter Randomized Trial [V3; NCT01059175; Bordachar P et al. J Card Fail 2010].
This recently completed clinical trial involving 100 patients was designed to determine whether TriV pacing will significantly improve outcomes in nonresponders in terms of clinical and echocardiographic endpoints. The primary endpoint was the comparison of the proportion of patients improved, unchanged, or worsened at 12 months. Although final data are not yet available, Prof. Leclercq stated that there were no reports of failed implantation of the new LV lead.
Overall, he concluded that TriV pacing significantly improves LV reverse remodeling compared with conventional BiV pacing. Although the clinical relevance of TriV pacing requires further evaluation in randomized clinical trials, he hopes emerging data from the V3 trial will provide more insight into its effects in patients who are nonresponders to conventional CRT.
Mauro Biffi, MD, University of Bologna, Bologna, Italy, discussed that although LV endocardial pacing has been reported to improve HF status and LV function in case reports or small series due to increased flexibility in LV site selection, it is associated with complications such as thromboembolic disorders.
He also discussed a guided approach to LV lead placement, including an ongoing pilot study enrolling patients who have failed CRT implantation by a conventional tranvenous approach or patients that have failed to respond to CRT, using a more integrated and individualized approach to therapy. Pivotal to achieving the maximum benefit from LV endocardial stimulation is locating the site of latest mechanical activation by imaging techniques [Doring M. Europace 2013] or by acute hemodynamic testing [Derval N. J Am Coll Cardiol 2010]. After locating the site of latest mechanical activation by 3D echocardiography, coronary sinus angiography is used to target the correct vein. Despite the potential to improve responder rate, the procedure requires transesophageal or intracardiac echocardiography assistance, thus resulting in relevant costs compared to conventional CRT implantation.
Prof. Biffi summarized by saying that regardless of the technique used to approach the LV, it should target the spot most likely to result in optimal LV mechanical improvement. And additionally, the most important requirement for the advancement of CRT lies in imaging equipment which will allow an individualized approach to LV stimulation.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.